A 2026 benchmarking and regulatory guide for pediatric practice administrators, physician-owners, revenue cycle directors, and financial leaders of medical groups that provide pediatric services.
Executive Summary
Pediatric practices enter 2026 facing a revenue cycle environment unlike any other specialty's — one where the dominant financial risk is not a fee schedule cut, but the stability of the coverage itself. Medicaid and CHIP cover a very large share of America's children, and the One Big Beautiful Bill Act (OBBBA, P.L. 119-21) is now contracting that payer base through work requirements, six-month redeterminations, shortened retroactive coverage, and narrowed eligibility. Layer on the most volatile childhood vaccine policy environment in three decades and a payer adjudication apparatus that is increasingly automated, and the practices that stay profitable will be the ones that treat revenue cycle management as a strategic asset, not a back office.
The defining macro-theme of 2026: eligibility is the new denial frontier.
In surgical specialties, the revenue fight happens at prior authorization and coding. In pediatrics, it increasingly happens before the visit even occurs — in whether the child's Medicaid coverage survived the last redetermination cycle, whether the newborn was added to the policy in time, and whether the vaccine administered last Tuesday is still on the payer's covered list. The operational answer is the same in every case: verification infrastructure, built now, before the January 2027 convergence hits.
The six developments pediatric financial leaders must understand:
1. The OBBBA Medicaid contraction is a pediatric revenue event. KFF's analysis of CBO-based estimates puts the federal Medicaid spending reduction at $911 billion over 2025–2034, while CBO's Medicaid chapter reports $886.8 billion in deficit reduction and 7.5 million more uninsured people in 2034 from Medicaid provisions. Children are exempt from work requirements, but family-level renewal paperwork, caregiver disenrollment, and administrative churn can still create pediatric eligibility risk. Practices should treat parental reporting requirements as an indirect pediatric revenue-cycle risk.
2. Late 2026 and early 2027 are the convergence period: six-month redetermination requirements begin after Dec. 31, 2026, while work requirements and retroactive-coverage limits take effect at the start of 2027. Eligibility operations must be rebuilt during 2026.
3. Vaccine policy is in flux — but the money has not moved yet. The revised childhood immunization schedule HHS released January 5, 2026, is blocked by a federal district court order and is not currently in effect. The Vaccines for Children (VFC) resolutions are unchanged, HHS has stated previously recommended immunizations remain covered by Medicaid, CHIP, VFC, and Marketplace plans without cost-sharing, and several insurer groups have issued no-cost vaccine coverage commitments; AHIP-member plans have pledged no-cost coverage for ACIP-recommended immunizations through 2027, while practices should still verify payer-specific coverage rules.
4. CPT 2026 creates a reporting pathway for the vaccine conversation. New codes 90482–90484 allow reporting of standalone immunization counseling when no vaccine is administered, subject to payer coverage and documentation rules — a direct answer to the hesitancy-driven visits pediatricians have absorbed for free. Pair them with the restructured COVID-19 administration codes (90480 revised to "first or only component," new add-on +90481 for each additional component) and the RSV monoclonal antibody administration codes (96380/96381). JW/JZ requirements are not new, but practices should confirm payer-specific enforcement for single-dose injectable products, including RSV monoclonal antibodies, and ensure claims carry JW when there is discarded drug or JZ when there is none.
5. The CY 2026 Physician Fee Schedule tilts toward pediatrics — where it applies. The –2.5% "efficiency adjustment" that is compressing surgical specialties explicitly exempts time-based codes: E/M, care management, and behavioral health — the core of pediatric billing. With conversion factors rising to $33.57 (QP) and $33.40 (non-QP), practices whose Medicaid programs and commercial contracts benchmark to Medicare RVUs see a relative tailwind.
6. CMS-0057-F gives pediatrics enforceable prior-auth timelines with its dominant payers. Effective January 1, 2026, Medicaid managed care and CHIP managed care plans must decide on complete prior-auth requests within 72 hours (urgent) or 7 calendar days (standard) and provide specific denial reasons, with public reporting of approval and turnaround metrics beginning March 31, 2026.
Three priorities for the next quarter: (1) move eligibility verification from scheduling-time to day-of-service, every visit, every patient, before the 2027 redetermination cadence doubles churn; (2) operationalize 90482–90484 with modifier 25 discipline and time documentation, and audit every vaccine claim for product-administration pairing, component counting, and JW/JZ compliance; (3) shift performance management from clean claim rate to first pass resolution rate with a 90%+ target.
Pediatric RCM 2026, By the Numbers
In This Article
- What Is Driving 2026 Pediatric Revenue Pressure
- The OBBBA Medicaid Contraction
- The CY 2026 Fee Schedule and Pediatrics
- Vaccine Policy Volatility
- CMS-0057-F Prior Authorization Rules
- The 7 Must-Track Pediatric RCM KPIs
- How the Core Metrics Are Calculated
- Why FPRR Is the Gold Standard
- The Write-Off Trap
- CPT 2026 Changes That Hit Pediatrics
- Top Pediatric Denial Reasons & Prevention
- Using HFMA MAP Keys in Pediatrics
- Segmenting AR by Payer and Provider
- The Four Revenue-Integrity Mandates
- Urgent vs. Emerging
- Executive Checklist
- Frequently Asked Questions
- The Bottom Line
What Is Driving Reimbursement Pressure in Pediatric Revenue in 2026?
Four forces converged on pediatric revenue between mid-2025 and early 2026, and each one compounds the financial impact of eligibility gaps and slow workflows. Unlike the surgical specialties — where the pressure is concentrated in RVU compression and prior authorization — pediatric pressure is concentrated in payer-mix erosion and coverage verification. Understanding these forces is the context for every benchmark that follows.
The OBBBA Medicaid contraction: the pediatric payer base under pressure
Medicaid and CHIP cover nearly half of America's children, and Medicaid's EPSDT benefit guarantees comprehensive pediatric coverage through age 20. That makes federal Medicaid policy the single largest revenue variable for most pediatric practices — larger than any fee schedule, any coding change, and any commercial contract.
KFF's analysis of CBO-based estimates puts the federal Medicaid spending reduction at $911 billion over 2025–2034; CBO's Medicaid chapter reports $886.8 billion in deficit reduction and 7.5 million more uninsured people in 2034 from Medicaid. Children are exempt from work requirements, but family-level renewal paperwork, caregiver disenrollment, and administrative churn can still create pediatric eligibility risk. Practices should treat parental reporting requirements as an indirect pediatric revenue-cycle risk. Evidence from prior state-level work-requirement experiments shows coverage losses driven largely by administrative failure, not true ineligibility.
| Provision | Effective Date | Pediatric RCM Impact |
|---|---|---|
| Work requirements (80 hrs/month, expansion adults) | January 1, 2027 | Children are exempt, but parental procedural disenrollment and family-level renewal failures can create pediatric eligibility-verification risk; expect eligibility-related denials to spike in Q1 2027 |
| Six-month eligibility redeterminations (expansion adults) | Beginning December 31, 2026 | Doubles the annual churn cycles a family passes through; day-of-service eligibility verification becomes non-negotiable |
| Retroactive coverage cut: 3 months → 2 months (traditional Medicaid & CHIP), 1 month (expansion adults) | Applications on/after January 1, 2027 | Shrinks the window to rescue newborn and lapsed-coverage claims; services delivered before the retro window become permanent bad debt |
| Noncitizen eligibility narrowing: refugees, asylees, humanitarian parolees, and trafficking victims lose baseline eligibility; qualified-immigrant definition restricted largely to LPRs (5-year wait), Cuban/Haitian entrants, and COFA migrants | October 1, 2026 | Parents lose coverage while many children keep it under preserved CHIPRA 214 state options — a split-household verification problem, not a blanket self-pay conversion (see callout below) |
| Cost-sharing up to $35/visit (expansion adults, 100–138% FPL) | October 1, 2028 | Pediatric, primary care, preventive, emergency, and mental health services are explicitly exempt (as are FQHC/RHC services); harden billing edits to flag and appeal any MCO that improperly passes adult cost-sharing logic down to pediatric encounters |
| Provider tax safe harbor phase-down in expansion states: 6.0% → 5.5% in FY 2028, stepping to 3.5% by FY 2032 | FY 2028–2032 | Squeezes state Medicaid budgets; anticipate downstream pressure on pediatric Medicaid fee schedules and MCO rates |
The compounding factor: ACA's enhanced premium tax credits expired at the end of 2025, sharply increasing family premiums on the Marketplace. Families priced out of Marketplace coverage who don't qualify for Medicaid land in the self-pay column — and a member survey from the American Medical Group Association found 51% of physician organizations anticipating pediatric service reductions under the Medicaid cuts. Practices that build patient-pay infrastructure now — estimates, point-of-service collection, payment plans — will absorb the payer-mix shift; those that don't will watch it accumulate in A/R > 90.

The CHIPRA 214 carve-out: don't convert covered children to self-pay
Congress preserved the CHIPRA Section 214 state option, which lets states cover lawfully residing children and pregnant individuals with federal matching funds and without the five-year waiting period — and CMS guidance directs electing states to preserve that coverage even for children in the categories (refugees, asylees, parolees, trafficking victims) losing baseline eligibility on October 1, 2026. Many states — roughly three-quarters based on CMS's current state list — use the CHIPRA 214 option to cover lawfully residing children and/or pregnant individuals. The operational consequence is a split-household eligibility environment: beginning Q4 2026, a refugee or asylee parent may lose Medicaid entirely while their child remains fully covered under CHIPRA 214. Rewrite front-desk eligibility scripts for this scenario and never let a batch-eligibility failure on the parent's file auto-classify the child as self-pay — misclassifying covered immigrant children is preventable bad debt and preventable revenue leakage in equal measure.
The CY 2026 Physician Fee Schedule: a rare relative tailwind
CMS's CY 2026 Physician Fee Schedule Final Rule (CMS-1832-F) applies a –2.5% "efficiency adjustment" to the work RVUs of most non-time-based codes — but explicitly exempts time-based services: E/M, care management, and behavioral health. Those exempt categories are the core of pediatric billing.
For CY 2026, the conversion factors are $33.57 for qualifying APM participants (+3.77%) and $33.40 for non-qualifying clinicians (+3.26%), reflecting the statutory one-year 2.5% increase under OBBBA plus a 0.49% budget-neutrality adjustment. While Medicare itself is a small direct payer for pediatrics, the PFS matters enormously in the second order: many state Medicaid programs peg physician rates to a percentage of Medicare. Many Medicaid and commercial contracts reference Medicare RVUs, fee schedules, or relative-value methodologies, so the PFS can have second-order effects beyond Medicare's small direct role in pediatrics.
A strategic read: the 2026 PFS is relatively more favorable to E/M-heavy pediatric practices than to procedure-heavy specialties exposed to the efficiency adjustment. Practices should press it in commercial contract negotiations — an E/M-weighted case mix rides the rising conversion factor without absorbing the efficiency adjustment that is compressing surgical groups. If your contracts haven't been renegotiated since the 2026 values published, you are leaving that leverage unused. One housekeeping item with real dollars attached: the $0.17 spread between the QP and non-QP conversion factors looks trivial per claim, but multiplied across thousands of E/M encounters per provider per year, it aggregates into five figures — audit each clinician's Quality Payment Program status for 2026 and confirm the billing system is configured to project and reconcile against the correct rate.
Vaccine policy volatility: the coverage question of 2026
Vaccines are simultaneously a clinical cornerstone, one of the largest non-payroll expense lines in a pediatric practice, and — in 2026 — the most policy-volatile revenue category in ambulatory medicine.
The sequence matters for billing teams, but it should be framed as litigation-driven uncertainty, not as settled operating policy. In 2025 and early 2026, HHS/CDC and the newly reconstituted ACIP announced or voted on multiple pediatric vaccine changes, including COVID-19 shared clinical decision-making language, MMRV first-dose changes, hepatitis B birth-dose changes, and the January 5, 2026, revised childhood immunization schedule. However, on March 16, 2026, the U.S. District Court for the District of Massachusetts stayed the January 2026 memo, stayed the challenged ACIP appointments, and stayed all votes taken by the now-stayed ACIP. As a result, practices should not treat those stayed actions as current federal operating policy while the litigation proceeds. Billing, vaccine-inventory, and charge-capture workflows should remain aligned with the currently operative CDC/ACIP schedule, VFC guidance, and payer-specific coverage rules.
Here is what has not changed, and it is the operational anchor: because the court stayed the challenged January 2026 schedule changes and ACIP actions, practices should continue relying on the currently operative CDC/ACIP and VFC guidance, while verifying payer and VFC rules before changing inventory or billing workflows. HHS stated that all previously recommended immunizations remain covered without cost-sharing by Medicaid, CHIP, VFC, and Marketplace plans. And several insurer groups announced no-cost vaccine coverage commitments; AHIP-member plans have pledged coverage through 2027, while some earlier public commitments were framed through 2026. Practices should verify plan-specific coverage policies before changing vaccine inventory, billing, or charge-capture workflows.
Important note: the insurer's pledge is voluntary and time-limited. If narrowed recommendations are reinstated, new binding guidance is issued, or payer policies change in 2027, plans may begin differentiating coverage or documentation requirements, particularly for vaccines moved to shared clinical decision-making. Treat SCDM vaccine encounters as documentation-sensitive when required by the currently operative recommendation, payer policy, or clinical circumstances, and build the 2027 vaccine-coverage verification workflow during 2026, not after the first denial wave. Note the dual-pathway reality underneath: VFC eligibility and payer coverage algorithms key off ACIP resolutions, while clinicians may also look to AAP guidance when it diverges from payer interpretations, so billing operations should deliberately bridge that gap (see denial category 4 below).
CMS-0057-F: enforceable prior-auth timelines with pediatrics' biggest payers
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) is often framed as a Medicare Advantage story, but its impacted-payer list includes Medicaid managed care and CHIP managed care — which, for most pediatric practices, means the rule covers nearly the entire payer book. Effective January 1, 2026, impacted plans must complete prior-auth requests within 72 hours for urgent requests and within 7 calendar days for standard requests, and must provide specific, traceable denial reasons regardless of the submission channel. The first cycle of mandatory public reporting of approval, denial, and turnaround metrics came due March 31, 2026 — and this is the underused lever. Until this year, arguing that an MCO was slow-walking authorizations meant relying on internal anecdote; now every impacted plan's approval rates, denial rates, and average turnaround times are published. Pull that data, cross-reference it against your internal first-pass and turnaround experience with the same plan, and bring the discrepancies — in writing — to Joint Operating Committee meetings and 2027 contract renegotiations. A payer's federally mandated compliance data can be a strong negotiating exhibit in MCO escalations and 2027 contract discussions. FHIR-based Prior Authorization APIs follow on January 1, 2027, laying the groundwork for EHR-integrated authorization workflows.
Where pediatric prior auth bites hardest — behavioral and developmental health services, specialty referrals, durable medical equipment, and high-cost biologics like RSV monoclonal antibodies under some plans — those compressed windows only help if the submission is complete on the first pass. Incomplete submissions reset the clock.
What Are the Must-Track Pediatric RCM KPIs in 2026?
These seven KPIs, mapped, where applicable, to HFMA MAP Key domains and informed by MGMA/HBMA standards and pediatric RCM experience, form the recommended 2026 pediatric operating target set — the targets high performers actually hit, not merely "acceptable." Pediatric practices should benchmark at the aggressive end of every range: with a high-volume, low-dollar, E/M-weighted claim mix and comparatively light prior-authorization exposure, there are fewer structural excuses for slow or leaky revenue than in surgical specialties.
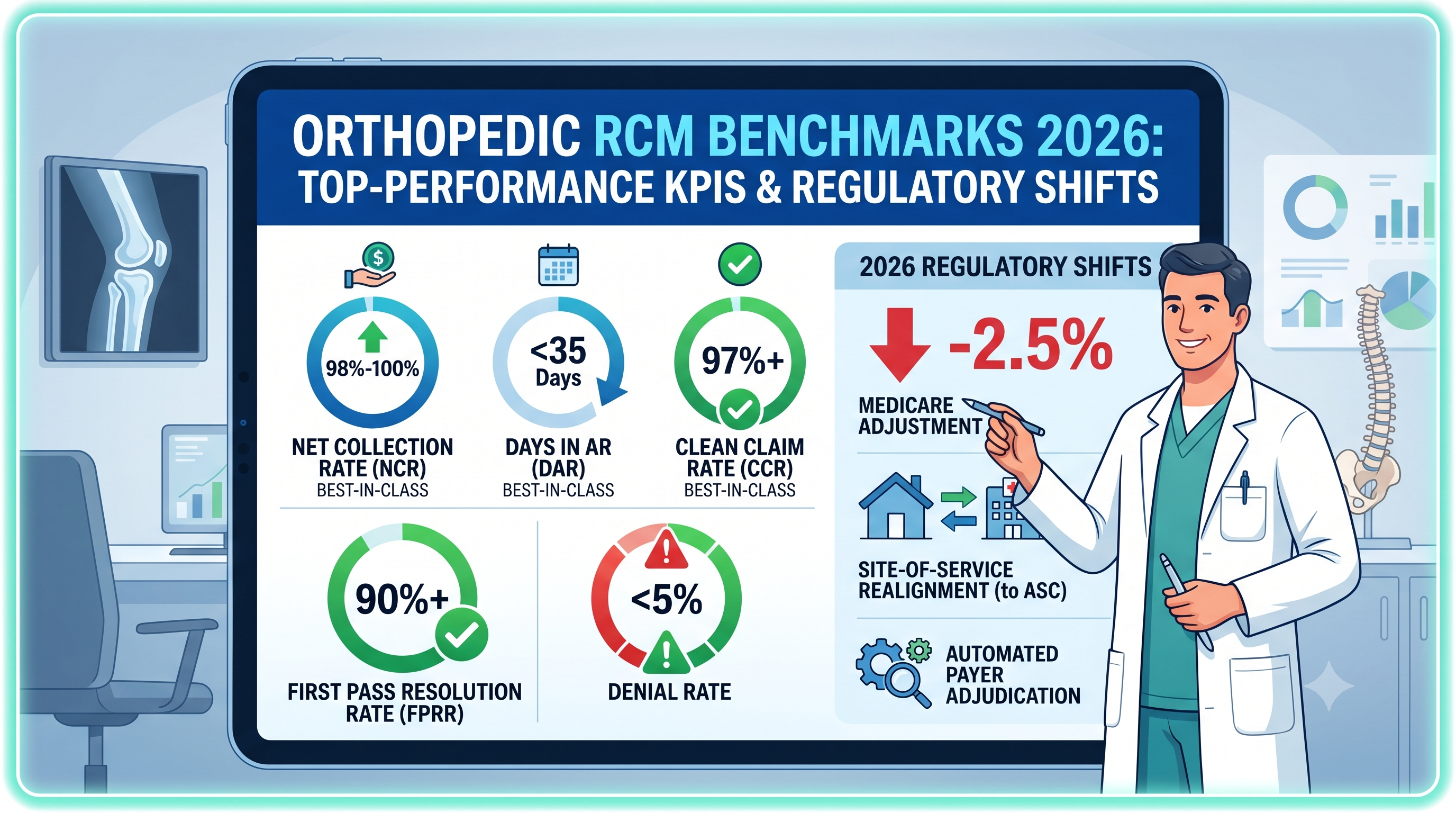
| Key Performance Indicator (KPI) | Best Practice (Top Performers) | Industry Average / Threshold | HFMA MAP Domain |
|---|---|---|---|
| Net Collection Rate (NCR) | 98% – 100% | ~95% (improvement threshold) | Financial Management |
| Revenue Realization Rate (RRR) | 99% – 100% (90 days in arrears) | 95% – 98% | Standalone Billing Integrity |
| Days in AR (DAR) | < 30 days (elite < 25) | 30 – 40 days | Account Resolution |
| Billed A/R > 90 Days | < 10% | 15% – 25% | Account Resolution |
| Clean Claim Rate (CCR) | 97%+ (elite 99%) | 85% – 90% | Claims & Pre-Billing |
| First Pass Resolution Rate (FPRR) | 90%+ (elite 95%) | 80% – 85% (below 75% needs review) | Claims & Pre-Billing |
| Denial Rate | < 5% (elite < 3%) | 9% – 12% | Account Resolution |

How Are the Core Pediatric RCM Metrics Calculated — and What Should They Hit?
Net Collection Rate (NCR)
NCR = total payments ÷ net charges (gross charges minus contractual adjustments). It measures the share of contractually allowed revenue you actually recover.
Performance at or below 95% signals leakage — in pediatrics, most commonly uncollected copays and deductibles on sick visits, unworked family balances spread across multiple sibling accounts, and vaccine product dollars lost to billing errors. Target 98%–100%. Pediatric margins are thin enough that a two-point NCR slip on a $3 million book is $60,000 — roughly the annual carrying cost of a substantial private vaccine inventory. And never trust NCR alone: it is the metric most easily inflated by misbooked write-offs (see the write-off trap below).
Revenue Realization Rate (RRR)
RRR = (total payments + all approved adjustments) ÷ total gross charges. It is an integrity check confirming every gross-charge dollar is accounted for by payment or a valid adjustment.
Benchmark 99%–100%, calculated exactly 90 days in arrears — running it in real time distorts the results due to payer adjudication lag. In pediatrics, a rate below 99% typically points to charge-capture breakdowns concentrated in three places: vaccine administration codes dropped from the claim (the product billed without 90460/90461 or 90471–90474), screening instruments administered but never charged (96110, 96127, 96160/96161), and after-hours or weekend add-on codes omitted from urgent visits.
Days in Accounts Receivable (DAR)
DAR = total active billed AR ÷ average daily net patient service revenue, where the denominator is the most recent 3-month (90-day) average per the HFMA MAP Key standard.
Pediatric DAR should run lower than the all-specialty average: claims are numerous but simple, prior authorization is light, and Medicaid MCOs adjudicate electronically. The pediatric target is under 30 days, elite under 25 — a practice sitting at 40+ days has a workflow problem, not a specialty problem. Exclude patient credit balances (endemic in pediatrics thanks to family prepayments and duplicate copay collection), unbilled (DNFB) accounts, and bad debt already placed with collectors. The most effective operational lever is same-day charge capture: well visits and sick visits should drop to the clearinghouse within 24 hours.
Billed A/R > 90 Days
Billed A/R > 90 = billed receivables aged beyond 90 days ÷ total active billed A/R, excluding DNFB, placed bad debt, and credit balances. It isolates the "stuck" revenue most likely to become bad debt.
The pediatric aging tail is built from different material than a surgical practice's: retro-eligibility claims awaiting Medicaid application outcomes, newborn claims held pending policy enrollment, coordination-of-benefits disputes between two parents' plans, and family self-pay balances. The HFMA standard is under 10%. Track self-pay A/R > 90 separately against its own threshold (under 30%) and expect that segment to grow as OBBBA coverage losses and Marketplace premium increases push more families into self-pay.
Clean Claim Rate (CCR) and First Pass Resolution Rate (FPRR)
CCR = clean claims ÷ total submitted (pass formatting edits without manual intervention). FPRR = claims paid on first submission ÷ total submitted — adjudicated and paid, no rework.
CCR is a front-end formatting metric. Common pediatric failures include missing or mismatched vaccine product-administration pairs, the wrong administration code family for the payer (VFC vs. private stock), missing Z23 linkage, and preventive codes billed outside the payer's age or frequency window. Target CCR 97%+ (elite 99%). But a clean claim is not a paid claim, which is why FPRR matters more (next section).
Denial Rate
Denial Rate = denied claims ÷ total submitted. Track both the initial denial rate (front-end accuracy) and the final denial rate (permanent loss after appeals).
Published industry data put national initial denial rates at around 11.8% in 2024. Pediatric practices should target under 5%, with under 3% representing elite performance. In pediatrics, distinguish claim-level from line-item denials with particular care: a rejected $18 vaccine administration line can flag a $400 well-visit encounter as "denied" and distort reporting — and because pediatric denials are individually small, teams under volume pressure quietly stop working them, converting a reporting nuisance into permanent leakage.
Why Is FPRR the Gold Standard, Not Clean Claim Rate?
First-pass resolution rate is the truer efficiency measure because it tracks claims all the way to payment, whereas clean claim rate stops at submission. A claim can pass every formatting edit and still be denied for eligibility, coverage, or documentation.
A well-configured scrubber can produce a high clean-claim rate while the practice still underperforms on first-pass resolution. In pediatrics the gap between the two metrics is dominated by exactly one category: eligibility. The claim was formatted perfectly — but the child's Medicaid coverage lapsed at redetermination, the newborn was never added to the parent's plan, or the family's MCO assignment changed on the first of the month. No scrubber edit catches a coverage change that happened after the eligibility file was pulled. Industry sources report that a substantial share of denied claims is never resubmitted, with estimates commonly ranging from roughly one-third to 60% or more, depending on setting and methodology, converting preventable denials into permanent leakage. Manage to FPRR with 90%+ as the working target and 95%+ as best practice; treat CCR as an upstream control, not the finish line. A dedicated AR and denial management operation exists precisely to close the gap between the two numbers.
The financial overhead of a denial is its own argument for front-end accuracy — and pediatric economics make the math harsher, not gentler:
| Claim Processing Stage | Avg. Cost per Claim | Pediatric Reality Check |
|---|---|---|
| Initial electronic claim submission | $3 – $6.50 | Manageable at pediatric claim volumes when fully electronic |
| Physician-practice denial rework/appeal | ~$25 | Frequently exceeds the value of the denied line itself — a $25 rework on an $18 vaccine administration line is a guaranteed loss either way |
| Broader denial rework estimates | $57 – $103 | At these costs, reworking a typical pediatric sick-visit denial consumes most or all of its collectible value |
This is the structural difference between pediatric and surgical denial economics: an orthopedic group can afford to appeal a $10,000 surgical denial with a $100 rework cost. A pediatric practice cannot afford to appeal thousands of $40–$150 denials at $25–$100 each. In pediatrics, denial prevention is not merely preferable to denial management — denial management is frequently uneconomic. The only winning strategy is a first-pass game: real-time eligibility at check-in, automated vaccine pairing edits, and payer-specific frequency rules enforced in the EHR templates before the claim is born. A practice submitting 2,000 claims per month at a 10% denial rate generates 200 denials; even at the conservative $25 physician-practice rework figure, that is $5,000 per month in administrative burn chasing balances that are often not worth the chase.
The Write-Off Trap: How a High NCR Can Mask Real Losses
When billing teams face backlogs of aged, denied, small-dollar claims — the default condition of an understaffed pediatric billing office — administrative write-offs get misclassified as contractual adjustments. This structural accounting error shrinks the net-charges denominator and artificially inflates NCR toward 100%, masking underlying leakage that healthcare financial audits frequently estimate at 3% to 5% of annual collectible revenue.
Contractual adjustments are planned, legally binding reductions to the payer's allowed amount — not losses. Administrative write-offs are permanent losses from operational failures: timely-filing lapses, eligibility gaps that never get resolved, denials that never get worked. Pediatrics is unusually vulnerable to the trap precisely because the individual amounts are small — writing off a $45 denied claim "to contractual" feels harmless in a way that writing off an $18,000 surgery does not. At pediatric volumes, the harmless-feeling entries add up to six figures.
| Scenario | Billed | Contractual Adj. | Admin Write-Off | Cash Collected | Reported NCR |
|---|---|---|---|---|---|
| Well visit + vaccines, paid clean | $650 | $280 | $0 | $370 | 100% (true) |
| Denied for lapsed eligibility — properly booked | $650 | $280 | $370 | $0 | 0% (true) |
| Denied — the write-off trap | $650 | $650* | $0 | $0 | 100% (inflated) |
*The $370 loss is misclassified into the contractual-adjustment column, zeroing out net charges and reporting a perfect collection rate on a claim that collected nothing — including the vaccine product dollars the practice paid for out of inventory.
How to catch it: monitor the adjustment-to-charge ratio by payer. A Medicaid-heavy pediatric mix runs a structurally higher contractual-adjustment percentage than a commercial-heavy book — so don't borrow another specialty's band; establish your own trailing-twelve-month baseline by payer category and set an alarm for deviations. A sudden, unexplained spike means collectible claims are being written off. Enforce a governance rule: any non-contractual write-off above a threshold (e.g., $100 in a pediatric book) requires supervisor approval and documented justification — and vaccine-product dollars always get worked, because that money already left the practice as inventory cost. This is a core discipline of professional revenue cycle management.
What CPT 2026 Coding Changes Hit Pediatrics Hardest?
The CPT 2026 set focuses its pediatric-relevant changes on immunization services — new reporting and potential payment pathways for counseling, new administration codes for new product classes, and stricter enforcement mechanisms. Five updates require immediate revisions to the template and charge sheet.
| Code(s) | Service / Description | Key Coding Mandate | Denial Risk to Manage |
|---|---|---|---|
| 90482 – 90484 (new) | Standalone immunization counseling when no vaccine is administered same day; 90482 = 3–10 min (0.24 wRVU), 90483 = >10–20 min (0.50 wRVU), 90484 = >20 min (0.75 wRVU); one code per patient per date | Time-based; documentation must show total counseling time distinct from other services (time counseling on vaccines actually administered is excluded); pair with Z71.85 and the applicable Z28.xx refusal code; reportable via telehealth where permitted by payer, program, and state telehealth rules | When billed with a same-day E/M, modifier 25 must be appended to the E/M; missing time documentation and missing modifier 25 are the dominant denial patterns — and payer adoption is uneven, with some plans placing the codes on nonpayment lists, so verify coverage payer-by-payer before go-live |
| 90480 / +90481 | COVID-19 administration restructured: 90480 revised to "first or only component of each vaccine administered"; +90481 is a new add-on for each additional component | Reportable only when the vaccine includes a COVID-19 component; flu-COVID combination products (90612/90613, lightning-bolt codes pending FDA approval) would be reported with 90480 + 90481 | Do not treat these as generic combo-administration codes — charge templates must enforce the component logic, and lightning-bolt product codes must not be billed before FDA/CDC status resolves for the product in hand |
| 96380 / 96381 | RSV monoclonal antibody administration — nirsevimab (Beyfortus) and clesrovimab (Enflonsia) | 96380 with counseling, 96381 without; link product and administration to Z29.11 | JW/JZ requirements are already in effect for applicable separately payable single-dose drugs; missing modifiers can cause claims to be returned, rejected, or denied depending on payer and program rules |
| 90460 / 90461 vs. 90471 – 90474 | Counseling-based (through age 18) vs. non-counseling administration families | Component counting on 90461 must match the combination product's antigen count; every product code pairs with an administration code linked to Z23 | Missing 90461 component units and dropped administration lines remain the highest-volume pediatric coding error; payers also police counseling documentation supporting the 90460 family |
| Preventive E/M frequency edits (99381–99385 / 99391–99395) | Age-banded preventive visit codes | Age on date of service governs code selection; payers are enforcing stricter age cutoffs and minimum intervals between annual visits | Billing even days early against a payer's frequency rule triggers rejection or downcoding — align recall scheduling with payer-specific frequency logic |
The opportunity hiding in 90482–90484: pediatricians have absorbed vaccine-hesitancy conversations as unpaid work for years. These codes create a potential payment pathway for that time — including via telehealth where permitted — but only for practices that build the documentation and payer-specific workflow: a discrete time field in the note template, an order-entry prompt when a recommended vaccine is declined or deferred, and a charge-router rule that appends modifier 25 when an E/M shares the date. Payer adoption will be uneven through 2026; track remittances by payer and escalate non-payment with the AAP's payment advocacy materials. Specialty-fluent clinical coding support pays for itself fastest in exactly this kind of transition year.
One further documentation shift worth engineering into templates: documented social risk factors can support E/M medical decision-making when they significantly limit diagnosis or treatment, and the note connects the risk factor to the management plan. Do not count Z55–Z65 codes alone unless the documentation supports their impact on care. When the Z code is documented but never tied to a management decision, payers reduce the level. In a specialty where undercoding sick visits is endemic, that linkage discipline is real money.
What Are the Top Pediatric Denial Reasons — and How Do You Prevent Them?
Pediatric denial patterns look nothing like surgical ones. Prior authorization and medical necessity — the surgical killers — are secondary here. Four categories account for most preventable pediatric losses, and each is a front-end problem.
1. Vaccine billing errors
Vaccine claims are the most error-dense category in pediatric billing because a single injection generates a multi-line claim with strict pairing logic: product code, administration code, component counting, diagnosis linkage, and now waste modifiers. The recurring failures — a product billed without its administration line, 90461 units that don't match the combination product's antigen count, missing Z23 linkage, VFC-stock doses billed as private stock (or the reverse), and absent JW/JZ modifiers on single-dose injectables — each individually small, collectively material. Because vaccines are also among the largest non-payroll expense lines in a pediatric practice, a denied vaccine claim is a double loss: the reimbursement and the inventory dollars already spent. Build automated claim edits that refuse to release any vaccine product line without its paired administration line, correct units, correct stock designation, and correct modifiers.
2. Eligibility churn and newborn coverage gaps
Eligibility-related denials are likely to become a larger pediatric denial driver as redetermination and reporting requirements tighten, and the trajectory is set: six-month redeterminations for expansion adults begin December 31, 2026, work requirements land January 1, 2027, and the retroactive coverage window shrinks to two months (traditional Medicaid and CHIP) or one month (expansion adults) for applications filed on or after January 1, 2027. Newborn claims deserve their own workflow because the retro-coverage compression collides with fragile state-level newborn billing mechanics. Many state Medicaid programs instruct providers to bill a healthy newborn's services under the mother's Medicaid ID for roughly the first 30 days of life before a unique infant ID is issued; commercially, the coordination-of-benefits "Birthday Rule" decides which parent's plan is primary when both carry coverage. Every day lost to a Birthday Rule dispute or a delayed state ID assignment now burns down a shorter retroactive window — and Medicaid MCO timely-filing limits as short as 120 (sometimes 90 or 60) days mean aged newborn claims can no longer count on long-tail retroactive approvals for rescue. The working standard: resolve COB and secure the infant's own Medicaid ID before day 45 of life, so claims finalize well inside both the retro window and the filing clock. The prevention program: real-time eligibility verification at every check-in rather than at scheduling; a monthly re-verification sweep of the active Medicaid panel to catch redetermination losses before the next visit; a newborn-enrollment tracking queue with claims held until coverage is confirmed; and front-desk scripts that tell families exactly what a redetermination notice looks like and what to do with it.
3. Same-day preventive plus sick visits, and screening bundling
The classic pediatric modifier problem: a well visit that surfaces a genuinely separate problem — otitis media found during the physical, an asthma exacerbation addressed with a medication change — supports a problem-oriented E/M billed alongside the preventive code with modifier 25. Payers deny these at high rates when the documentation doesn't show a distinct assessment and plan, and some routinely bundle them regardless, requiring an appeal with notes. The parallel pattern is screening bundling: 96110 (developmental screening with a validated instrument such as ASQ-3 or M-CHAT-R), 96127 (brief emotional/behavioral assessment), and 96160/96161 (health risk assessments) are separately billable with proper documentation, and payers vary widely on units and frequency. Prevention is template-level: separate documentation blocks for the preventive and problem-oriented portions, and a payer-specific screening matrix maintained quarterly.
4. Coverage ambiguity from vaccine schedule volatility
New in 2026: denials may arise not from coding error, but from coverage uncertainty created by stayed federal actions, divergent clinical guidance, and payer-specific system loading. Because the March 16, 2026, court order stayed the challenged January 2026 schedule changes and ACIP votes, practices should not assume the MMRV or hepatitis B changes are current federal operating policy while the stay remains in effect. The prevention posture: verify vaccine benefits by payer rather than assuming schedule-wide coverage; document shared clinical decision-making only where the currently operative recommendation, payer policy, or clinical documentation supports it; keep charge templates aligned with operative CDC/ACIP/VFC guidance; and monitor remittances for new documentation-request patterns that may signal payer tightening ahead of 2027. Where AAP clinical guidance and payer interpretation diverge, build a standing appeal template that cites the current AAP recommendation, the clinician's documented medical decision-making, and, when relevant, the family's preference.
The EPSDT shield: pediatrics' structural protection
Medicaid's Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) benefit legally guarantees comprehensive coverage of medically necessary services for enrolled children and adolescents through age 20, a mandate that survives OBBBA. When a Medicaid MCO denies a pediatric service on coverage or necessity grounds, EPSDT is frequently the winning appeal argument because the MCO's obligation extends beyond its commercial benefit templates. Revenue cycle teams that cite EPSDT explicitly in pediatric Medicaid appeals and that know the state's EPSDT periodicity schedule could overturn denials that generic appeal letters lose. The OBBBA cost-sharing provisions arriving in 2028 also explicitly exempt pediatric and primary care services: know these protections and use them in payer disputes.
How Should Pediatric Leaders Use HFMA MAP Keys?
The HFMA MAP Keys are 29 standardized KPIs across five domains — Patient Access, Pre-Billing, Claims, Account Resolution, and Financial Management — with consistent definitions that let a practice benchmark against national peers using the same math.
For pediatric groups inside larger multispecialty organizations or health systems, their value is definitional discipline: report pediatric performance against MAP Key definitions at the service-line level, so a strong system-wide average can't mask an underperforming pediatric line — or, just as commonly, so a high-performing pediatric line gets credit instead of subsidizing surgical inefficiency invisibly. Four keys deserve pediatric priority:
Insurance Verification Rate (PA-3): the single most important MAP Key for pediatrics in the OBBBA era. Encounters with electronic eligibility/benefits verification — target effectively 100%, executed day of service, because the redetermination cycle can invalidate last week's verification.
Pre-Registration Rate (PA-2): scheduled encounters pre-registered before service. In pediatrics, this is where problems with newborn enrollment status, MCO reassignment, and guarantor/custody data are caught before they result in denials.
Days in DNFB (PB-1): claims-generation timing — best practice 3–5 days. Pediatric encounters are short and template-driven; there is no defensible reason for well-visit charges to sit unbilled.
Total Charge Lag Days (PB-4): encounter-to-submission time. Enforce a 24-hour chart-closure standard; in a specialty of high claim counts and small balances, cash velocity is a volume game.
How Should Pediatric Practices Segment AR by Payer and Provider?
Segment AR aging by both payer category and individual provider. A single consolidated number conceals localized bottlenecks — a slow MCO, timely-filing risk, and credentialing lags on newly hired clinicians.
Payer segmentation and timely-filing risk
Separate self-pay from insurance AR, then split insurance into Medicaid FFS, each Medicaid MCO individually, CHIP, commercial, and Marketplace plans. The MCO-level split matters because Medicaid managed care plans within the same state can differ dramatically in denial behavior, timely-filing windows (some as short as 90 or even 60 days), and vaccine payment policy — and the CMS-0057-F public reporting that began March 31, 2026, now gives you comparative approval and turnaround data to bring to those conversations. Work each aging bucket to a defined action:
| Aging Bucket | Operational Focus | Risk | Recommended Collection Action |
|---|---|---|---|
| 0–30 days | Confirm claim receipt and adjudication status | Minimal | Review clearinghouse rejections daily; correct demographic, subscriber, and vaccine-pairing errors at the source |
| 31–60 days | Resolve eligibility and COB issues | Low | Chase newborn enrollment confirmations; resolve two-parent coordination-of-benefits and birthday-rule disputes; re-verify MCO assignment |
| 61–90 days | Work coding and bundling denials | Moderate | Appeal modifier-25 and screening-bundling denials with documentation; batch-appeal identical vaccine denials per payer, rather than working them one-off |
| 91–120 days | Formal appeals: escalate systemic payer issues | High | Escalate claims near short MCO filing limits; invoke EPSDT in Medicaid necessity appeals; escalate patterned MCO behavior with CMS-0057-F public metrics in hand |
| 120+ days | Forensic review; self-pay resolution | Critical | Identify systemic payer delays; resolve retro-eligibility claims before the 2027 window compression; route exhausted family balances to compassionate but structured collection workflows |
Provider credentialing segmentation
A major source of pediatric high-dollar aging is the onboarding of new pediatricians, NPs, and PAs — and pediatrics adds a wrinkle: the new clinician must be credentialed not just with commercial plans but with each Medicaid MCO individually, and enrolled in the state's VFC program before administering VFC stock. Billing before credentialing finalizes leaves claims rejected or held indefinitely; once they pass timely-filing limits, the loss is permanent. Segment the aging report by billing provider to isolate credentialing-held claims, prevent premature submission, and hold credentialing coordinators accountable. Initiate credentialing 90 to 120 days before a clinician's start date, with VFC enrollment on the same critical path.
The Four Revenue-Integrity Mandates for 2026
To insulate pediatric margins from coverage churn and payer automation, practice leaders should execute four operational mandates now. (For the broader technology playbook, see our companion guide on 18 technologies and strategies driving 2026 practice revenue growth.)
1. Move eligibility verification to day-of-service, every visit. Scheduling-time verification was adequate in an annual-redetermination world. It is obsolete in a six-month-redetermination world with work-requirement churn arriving January 2027. Deploy real-time eligibility at check-in, run a monthly re-verification sweep of the active Medicaid panel, and stand up a newborn-enrollment tracking queue. Measure against MAP Key PA-3 with a target of effectively 100%.
2. Shift benchmarks from CCR to FPRR. Establish a 90%+ first-pass target (95% top-decile) and audit the baseline gap between the two metrics. In pediatrics that gap is an eligibility report card: a practice holding 98% CCR against 80% FPRR does not have a coding problem — it has a coverage-verification problem, and the fix is upstream.
3. Harden the vaccine revenue line. Automated edits enforcing product-administration pairing, 90461 component counts, VFC/private stock designation, Z23/Z29.11 linkage, and JW/JZ modifiers; a quarterly reconciliation of doses administered (from the EHR immunization module) against doses billed and doses purchased; and an operational rollout of 90482–90484 with time-field documentation and modifier-25 routing. Vaccine inventory is prepaid revenue — treat vaccine inventory leakage as a direct margin loss, not a minor coding issue.
4. Establish a 24-hour chart-completion standard. Aligned with HFMA MAP Key PB-4: pediatric encounters are template-driven and short, so charge lag is a discipline problem, not a complexity problem. Same-day closure protects DNFB, compresses DAR, and keeps the high-volume/low-dollar cash engine turning. Practices without the internal bandwidth to run all four mandates concurrently should consider specialty-fluent medical billing services rather than entering 2027 unprepared for the 2027 deadlines.
Urgent vs. Emerging: Where to Focus First
Act Now (next 90 days)
Day-of-service eligibility verification — deployed and measured before redetermination frequency doubles.
90482–90484 go-live — time documentation, modifier-25 routing, payer remittance tracking.
JW/JZ compliance on single-dose injectables — requirements are already in effect for applicable separately payable drugs, and missing modifiers can cause claims to be returned or denied.
Vaccine coverage verification by payer — stop assuming schedule-wide coverage; document shared clinical decision-making when required by the currently operative recommendation, payer policy, or clinical circumstances.
Charge template hygiene — reconcile immunization templates against the currently operative CDC/ACIP schedule, VFC guidance, and payer-specific coverage rules. Track the stayed hepatitis B birth-dose and MMRV actions as litigation risks, but do not build templates as if those changes are current federal operating policy unless the stay is lifted or new binding guidance is issued.
QP/non-QP status audit — confirm each provider's 2026 Quality Payment Program status and that the billing system reconciles against the correct conversion factor.
Monitor & Prepare (2026 into 2027)
The January 2027 convergence — work requirements, six-month redeterminations, and the retroactive-coverage compression; model the payer-mix scenario now.
Vaccine coverage uncertainty — AHIP-member plans have pledged no-cost coverage through 2027, but payer-specific rules, state requirements, and litigation outcomes should be monitored.
FHIR Prior Authorization APIs (January 1, 2027) — plan EHR integration so authorization checks ride the API rather than portals and faxes.
State budget responses — provider-tax phase-downs begin pressuring state Medicaid budgets in FY 2028; watch your state's pediatric fee schedule and MCO rate-setting for early signals.
Marketplace family-coverage erosion — enhanced premium tax credits expired at the end of 2025; expect continued self-pay growth and invest in patient-pay infrastructure accordingly.
Executive Checklist: Pediatric Revenue Integrity for 2026
| Action | Owner | Timeframe | Strategic Impact |
|---|---|---|---|
| Deploy day-of-service real-time eligibility at every check-in; add monthly Medicaid panel re-verification sweep | Front office / RCM lead | Next 90 days | Neutralizes the largest 2026–2027 denial category before redetermination frequency doubles |
| Stand up a newborn-enrollment tracking queue with claim holds until coverage confirms | Billing manager | Next 90 days | Protects the claim category most exposed to the 2027 retroactive-coverage compression |
| Operationalize 90482–90484: time fields in templates, modifier-25 charge routing, payer remittance tracking | Coding lead / EHR analyst | Next 60 days | Creates a payer-dependent revenue opportunity for previously unpaid vaccine-hesitancy counseling |
| Build vaccine claim edits: product-administration pairing, 90461 component counts, stock designation, Z23/Z29.11, JW/JZ | RCM lead / clearinghouse admin | Next 90 days | Stops the highest-volume pediatric coding denials and protects prepaid inventory dollars |
| Quarterly reconciliation: doses administered vs. doses billed vs. doses purchased | Practice administrator | Quarterly, ongoing | Surfaces silent vaccine revenue leakage that NCR and CCR both miss |
| Rebase performance management on FPRR (90%+ target); audit the CCR-to-FPRR gap | Revenue cycle director | Next quarter | Redirects effort from formatting metrics to the eligibility failures costing money |
| Segment AR by individual Medicaid MCO; benchmark each against CMS-0057-F public metrics | Revenue cycle director | Next quarter | Arms MCO escalations and contract talks with the payer's own published performance data |
| Rewrite front-desk eligibility scripts for split-household immigrant coverage; block auto-classification of CHIPRA 214-covered children as self-pay | Front office manager / RCM lead | Before October 1, 2026 | Prevents covered immigrant children from being misclassified as self-pay when parents lose eligibility |
| Model the January 2027 payer-mix scenario (churn, retro-coverage, self-pay growth); size patient-pay infrastructure | CFO / physician-owner | By Q4 2026 | Converts the OBBBA convergence from a surprise into a budgeted, staffed transition |

Frequently Asked Questions
What are the most important pediatric RCM benchmarks for 2026?
The seven core benchmarks are: Net Collection Rate of 98%–100%, Revenue Realization Rate of 99%–100% measured 90 days in arrears, Days in AR under 30 (elite under 25), Billed A/R over 90 days under 10%, Clean Claim Rate of 97% or higher, First Pass Resolution Rate of 90% or higher (elite 95%), and a denial rate under 5% (elite under 3%). Pediatric practices should target the aggressive end of each range because their claim mix is high-volume, low-dollar, and E/M-weighted with light prior-authorization exposure.
How does the One Big Beautiful Bill Act (OBBBA) affect pediatric practices?
KFF's analysis of CBO-based estimates puts the federal Medicaid spending reduction at $911 billion over 2025–2034; CBO's Medicaid chapter reports $886.8 billion in deficit reduction and 7.5 million more uninsured people in 2034 from Medicaid provisions. Because Medicaid and CHIP cover a very large share of U.S. children, pediatric practices absorb this primarily as eligibility churn: six-month redeterminations for expansion adults begin December 31, 2026, work requirements start January 1, 2027, and retroactive coverage shrinks from three months to two months for traditional Medicaid and CHIP enrollees (one month for expansion adults) for applications filed on or after January 1, 2027. The revenue cycle answer is day-of-service eligibility verification, newborn enrollment tracking, and patient-pay infrastructure for families losing coverage.
Are children subject to Medicaid work requirements?
No. Children are exempt from OBBBA's work requirements, which apply to Medicaid expansion adults aged 19 to 64. However, parental reporting requirements can create indirect pediatric revenue risk when family paperwork, renewal timing, or caregiver disenrollment causes confusion or delays in a child's eligibility verification. That is why pediatric practices should treat parental work requirements as an indirect pediatric eligibility-verification risk beginning January 2027.
Do lawfully residing immigrant children lose Medicaid coverage under OBBBA?
Often not, even when their parents do. Effective October 1, 2026, federal Medicaid/CHIP matching is restricted for certain noncitizen categories, subject to CMS guidance and statutory exceptions. The change does not eliminate the CHIPRA 214 option for lawfully residing children and pregnant individuals, which lets states cover lawfully residing children and pregnant individuals with federal matching funds and without the five-year waiting period. Roughly three-quarters of states have elected the option, and CMS guidance directs those states to preserve coverage for CHIPRA 214-eligible children even in the categories losing baseline eligibility. The practical risk for pediatric practices is misclassification: a parent's eligibility failure should never auto-convert a covered child to self-pay status.
What are CPT codes 90482, 90483, and 90484 and how are they billed?
Effective January 1, 2026, CPT codes 90482–90484 allow reporting of standalone immunization counseling when no vaccine is administered, subject to payer coverage and documentation rules. They are time-based: 90482 covers 3 to 10 minutes (0.24 wRVU), 90483 covers greater than 10 to 20 minutes (0.50 wRVU), and 90484 covers greater than 20 minutes (0.75 wRVU). Only one code may be reported per patient per date, counseling time for vaccines administered is excluded, and claims should pair with ICD-10 codes Z71.85 and the applicable Z28.xx refusal code. Documentation must support the total counseling time as distinct from other services, the codes may be reported in person and, where permitted by payer, program, and state telehealth rules, via telehealth, and when billed alongside a same-day E/M visit, modifier 25 must be appended to the E/M code. Verify coverage payer by payer before go-live, as some plans have placed these codes on nonpayment lists.
Did the 2026 childhood vaccine schedule changes affect vaccine coverage and billing?
As of publication date, not yet, in payment terms. On March 16, 2026, a federal district court in Massachusetts issued preliminary relief in American Academy of Pediatrics v. Kennedy, staying the January 2026 CDC memo that revised the childhood immunization schedule, staying the appointments of 13 newly appointed ACIP members, and staying all votes taken by that now-stayed ACIP. As a practical result, the prior ACIP/CDC childhood immunization schedule is treated as back in effect while the litigation and appeal proceed; the court's action was a stay, not a final merit ruling. Because VFC coverage is tied to ACIP pediatric schedules and VFC resolutions, and because the court stayed the challenged ACIP actions, previously recommended pediatric immunizations generally remain available through VFC and continue to support no-cost coverage obligations under Medicaid/CHIP and ACA-compliant private and Marketplace plans, subject to applicable network and plan rules. AHIP-member health plans have pledged no-cost coverage for ACIP-recommended immunizations through the end of 2027, while practices should continue verifying payer-specific policy. Providers should continue documenting medical necessities, risk-based indications, and shared clinical decision-making where applicable, and should monitor payer bulletins, CDC/ACIP updates, and the pending litigation for any future coverage changes.
What is a good denial rate for a pediatric practice?
Best-in-class pediatric practices hold initial denial rates under 5%, with elite performers under 3%, against a national initial denial average of roughly 11.8% in 2024. Because pediatric claims are individually small, denial prevention matters more than denial management: rework costs of $25 to $103 per claim frequently exceed the collectible value of a denied pediatric line, so denials that would be appealed in a surgical practice simply become losses in a pediatric one.
Why is First Pass Resolution Rate more important than Clean Claim Rate?
Clean Claim Rate only measures whether a claim passed formatting edits at submission; First Pass Resolution Rate measures whether it was adjudicated and paid without rework. In pediatrics, the gap between the two is dominated by eligibility failures — coverage that lapsed at redetermination, newborns not yet enrolled, or mid-month MCO reassignment — none of which a claim scrubber can catch. Manage to an FPRR of 90% or higher, with 95% representing top-decile performance, and treat CCR as an upstream control rather than the finish line.
What is the write-off trap in pediatric billing?
The write-off trap occurs when administrative write-offs — permanent losses from operational failures like timely-filing lapses or unworked denials — are misclassified as contractual adjustments. This shrinks the net-charges denominator and artificially inflates Net Collection Rate toward 100% while real revenue leaks away, an error audits frequently estimate at 3% to 5% of annual collectible revenue. Pediatrics is especially vulnerable because individual balances are small enough that misclassification feels harmless. Catch it by tracking the adjustment-to-charge ratio by payer against your own trailing-twelve-month baseline and requiring supervisor approval for non-contractual write-offs above a set threshold.
How does the CMS prior authorization rule (CMS-0057-F) help pediatric practices?
CMS-0057-F applies to Medicaid managed care and CHIP managed care plans — the dominant payers for most pediatric practices. Effective January 1, 2026, those plans must decide complete prior-authorization requests within 72 hours for urgent cases and 7 calendar days for standard ones and must provide specific denial reasons. Mandatory public reporting of approval, denial, and turnaround metrics began March 31, 2026, giving pediatric groups comparative data to use in MCO escalations and contract negotiations, and FHIR-based Prior Authorization APIs arrive January 1, 2027.
How should pediatric practices prepare for the January 2027 Medicaid changes?
Prepare during 2026 on four fronts: deploy day-of-service real-time eligibility verification with a monthly re-verification sweep of the active Medicaid panel; build a newborn-enrollment tracking queue before the retroactive coverage window shrinks; model the payer-mix impact of parental churn and size patient-pay infrastructure for families losing coverage; and educate families proactively about redetermination paperwork so procedural disenrollments are caught before the next visit. Practices that wait until the first quarter 2027 denial wave will be repairing damage instead of preventing it.
The Bottom Line
The pediatric practices that stay financially strong into 2027 will treat revenue cycle management as a strategic asset, not a back office. The specialty's 2026 story is not a fee cut to absorb — it is a coverage base in motion, a vaccine policy environment in litigation, and a payer apparatus that automates faster than most billing offices adapt. The controllable levers are clear: verify eligibility at the door rather than at the schedule, manage to first-pass resolution rather than clean claims, defend the vaccine revenue line with automated pairing edits and quarterly reconciliation, cross-check NCR against the adjustment-to-charge ratio, and segment AR finely enough to catch a slow MCO or a credentialing lag before it bottlenecks cash. Benchmark your own numbers against your payer and patient mix first — then close the gap to top-decile, one KPI at a time.
Is Your Pediatric Revenue Cycle Ready for the 2027 Convergence?
Revele's revenue cycle specialists help medical practices benchmark their KPIs against top-decile performance, harden eligibility and vaccine-billing workflows, and turn their EHR workflows into denial-prevention engines — before the January 2027 Medicaid changes affect their payer mix.
Through the RISE Program, elite optimization services are now available to practices of every size.
Get a Complimentary Revenue Cycle Analysis →Disclaimer: The content published by Revele is provided for informational and educational purposes only and does not constitute legal, medical, financial, or tax advice. Healthcare laws, payer policies, coding rules, and compliance standards are highly complex and subject to frequent change. While Revele makes every effort to ensure that the information shared is accurate and up to date at the time of publication, we make no representations or warranties, express or implied, regarding the completeness or accuracy of this information.
Readers and users must consult with qualified professionals, certified coders, regulatory authorities, or independent legal and financial advisors for advice specific to their individual circumstances before making any strategic, clinical, coding, or operational decisions.
Benchmark ranges reflect MGMA, HFMA MAP Keys, and HBMA standards alongside 2025–2026 pediatric RCM reporting, including the CY 2026 Physician Fee Schedule Final Rule (CMS-1832-F), the AMA CPT 2026 code set, the CMS-0057-F Interoperability and Prior Authorization Final Rule, and the One Big Beautiful Bill Act (P.L. 119-21).