



Revenue Cycle Management

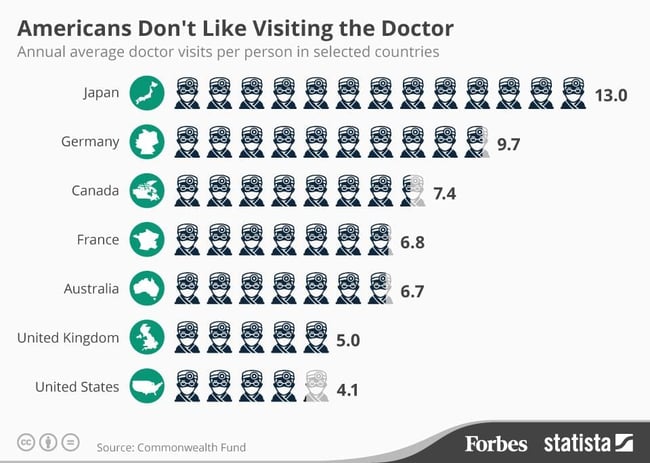
A trip to the doctor is fairly common in the United States. In fact, the average American visits a doctor four times per year. And when you do visit a doctor, it seems rather simple. You show up, check-in, describe what might be wrong or what’s going well, leave, and receive a bill on average 15 to 30 days later. But what you don’t see is the highly complex process taking place behind the scenes.
This highly complex process is revenue cycle management or, as some may call it, medical billing. And while the rising costs of healthcare may be front and center in today’s media, the process behind it, is not. But before we dive into the details of the revenue cycle management process, let’s take a look at why we bill for medical services.

Unlike other industries that receive payment at the time of service, healthcare is different. Statements are sent after the service is complete leaving patients with an obligation to take care of a cost they are typically unaware of before ever stepping foot into the exam room. But why?
Healthcare can be unpredictable. You may schedule an appointment for what seems like stomach pain but based on your exam, need an Xray or an additional appointment with a specialist. There are many factors that must be determined throughout your office visit that can lead to different levels of compensation for a provider.
It’s the medical billers job to ensure providers are compensated accurately based on the services performed. This is done by compiling information about the patient such as demographics, insurance coverage, and medical history along with the procedures performed by the physician during the office visit. All of this information is combined to create a claim.
Because there are typically multiple parties involved in a medical claim, the claims process quickly becomes quite complex, which lends itself to a variety of errors caused by both humans and technology. However, developing an efficient claims process is a common challenge when it comes to healthcare revenue cycle management.
Because the claims process begins before any claims are submitted, today's healthcare practices must have procedures in place that start the minute a patient contacts the office. From this point forward, practices must be prepared for all of the challenges that may come up during the claims process and develop processes to minimize these payment challenges.
By adhering to industry standards at all times, and developing procedures that are in line with the industry's best practices, healthcare administrators can create a claims process that works for the healthcare provider, the insurance company and the patient.
Underpaid, rejected or denied claims can cost your practice as much as $100,000 per month, according to the American Medical Association. And, if an insurance provider underpays a claim, statistics show that it is up to 35% lower than the original contract amount. Preventing claim errors is an ongoing effort for healthcare facilities but because healthcare costs are rising, insurance providers are in the business of carefully inspecting every claim that comes their way. This means that today, more than ever, providers are having a harder time getting paid for their services. There is always the potential to resubmit a claim, but resubmitting claims is time-consuming, costly, and typically doesn't happen within most revenue cycle management operations.
Preventing claim rejections not only prevents your practice from having to resubmit a claim, it can also speed up the time in which a claim is paid. So where do you start with preventing claim rejections? Understanding some of the most common administrative errors can help you develop workflows to prevent these types of claim rejections. These basic errors include:
To address these common errors, claims should be thoroughly proofread before they're submitted. Certain electronic health record (EHR) software systems will also have features that alert providers, medical coders, and medical billers when an error is present on a claim.
Efficient front office processes can often reduce the likelihood of a claim rejection due to patient demographic data but preventing rejections due to coding errors will require provider training on things like new CPT and ICD codes as well as ongoing training and coaching on proper documentation guidelines.
Having a Certified Professional Coder available to review claims, ensure coding accuracy, conduct internal audits, and provide ongoing training and education to providers is invaluable.
Preventing rejections is important but it is only half of the work required for an efficient claims process. After a claim is submitted, regular proper follow up with the insurance company on the status of the claim is critical. Through proper follow up, errors can be detected sooner and the claim can either be resubmitted or if it is denied, it can often be appealed.
Denied and rejected claims aren't identical. A rejected claim is returned because it contains errors, often simple clerical errors which can be corrected and a revised claim resubmitted.
It’s the medical billers job to ensure providers are compensated accurately based on the services performed. This is done by compiling information about the patient such as demographics, insurance coverage, and medical history along with the procedures performed by the physician during the office visit. All of this information is combined to create a claim.
A denied claim has been determined by the insurer to be unpayable, possibly due to missing information, but perhaps due to patient coverage. Denials can be successfully appealed, however studies show that once a claim is denied, many practices do not resubmit leading to most practices missing out on more than $75,000 per year in denied claims.
Don’t waste your time and your staff’s time with continuously reworking claims. Find out the source of the problem and prevent the denial in the first place. Being both proactive and reactive with your claims can result in a dramatic increase in your practice revenue.
Measure your practice’s denial data and find out the source of the denial. Identify the top three to five reasons for your practice’s denials and take action. Some of the most common reasons for claim denials include:
Neglecting to get pre-certification (or pre-authorization) can cost your practice and your patients money and can seriously decrease patient satisfaction.
Knowing which insurers require pre-authorization and for what is essential. In some cases your medical billing software can assist by flagging certain procedures and insurers so you'll know what to do. Additionally, it's better to get pre-authorization for a procedure that isn't ultimately done, rather than to do a procedure and try to get retroactive authorization for it.
Incorrect diagnosis and / or procedure codes can result in claim denials. While these situations can often be successfully appealed, again prevention is better. There's no substitute for well-trained coders and use of powerful medical billing software.
Different insurers impose different deadlines for claims submissions, and they have different policies about what you can do when you miss a deadline. In some cases, you can clear things up with a phone call, but in others you may have to fill out more paperwork.
You may be able to use your medical billing software to notify you of claims submission deadlines and procedures to follow when you miss one. In general, however, it's best to submit claims as soon as possible after services are rendered so your revenue cycle doesn't slow down.
Sometimes an insurer won't pay for a procedure it believes to be medically unnecessary. These can be difficult situations for all parties, but you may be able to avoid them. In any case where medical necessity isn't clear-cut, good communications among clinicians, medical billing staff, insurers, and patients is essential so everyone makes informed decisions.
When a claim is denied due to medical necessity, your practice could be forced to either absorb the cost of the services, or attempt to collect the entire payment from the patient, neither of which are good options.
Insurer networks can change from year to year, and patients may not realize this, or that changing insurance companies may change which medical providers they can see and receive full benefits. Ascertaining patient insurer information at the first opportunity (during appointment booking or registration) can allow your billing staff to determine whether your practice belongs to a patient's insurer network, and if not, what sort of benefits (if any) the patient can expect. Again, your medical billing software can assist with this by keeping you apprised of which networks your practice belongs to.
Less than 5 percent of claims should be denied on the first submission and your practice can make the necessary changes internally if denials are being caused due to practice errors. If payer errors are causing a high denial rate, you will need to make sure that your staff understands the payer’s reimbursement policies. Some payers publish guidelines regarding reimbursement. Your staff should be familiar with these guidelines to save time and effort by knowing when to appeal and when not to appeal a denied claim.
If you want to maximize your revenue cycle management, it's important to track at a minimum, the following medical billing key metrics and to measure them against the industry standards. Measuring is the first step in determining where your medical billing processes could use improvement.
The days in receivables outstanding is also known as days in accounts receivables. Days in Accounts Receivables (AR) is the average number of days it takes a practice to get paid. The lower the number the sooner claims are getting paid. Days in AR should be below the 30-40 day range. Monitoring your Days in AR will help to identify problems with a certain payer before it becomes unmanageable.
How to calculate: Total current accounts receivable (net of credits) divided by the average daily charge (12 previous months of gross charges divided by 365).
The industry standard DRO is 40-45 days; however, it is understandable that this may not always be achievable. By measuring this metric on a regular basis, you can determine what outside factors may contribute to your DRO and whether you need to make adjustments to your procedures based on the results of your measurements.
When measuring DRO, 40-45 is the norm. 45-64% indicates that your collections are slipping and over 65 days is considered problematic.
Of course, no practice wants to see receivables that are way overdue. However, in reality, having outstanding receivables that are over 120 days past due is common. The percentage of A/R over 120 days is a measure of the practice’s ability to get paid in a timely manner. This percentage represents the amount of receivables older than 120 days of the total current receivables. Although it isn’t the only aging indicator to evaluate, it is an excellent choice.
How to calculate: Take the dollar amount of your receivables, net of credits, that is greater than 120 days and divide that number by your total receivables, net of credits.
Having 15-18 percent of accounts receivable greater than 120 days is an acceptable performance indicator. However, if A/R>120 is greater than 25% it can be an indicator of poor performance.
The adjusted collection rate (also known as the net collection rate) is a measure of a practice’s effectiveness in collecting all legitimate reimbursement. This rate shows the percentage achieved out of the reimbursement allowed based on the practice’s contractual obligations. This figure reveals how much revenue is lost due to factors such as uncollectible bad debt, untimely filing and other non-contractual adjustments.
How to calculate: To calculate divide payments (net of credits) by charges (net of approved contractual adjustments) for a specific time frame. Ideally, the calculation should be based on matching the payments to the charges that created them in order to avoid fluctuations in results. If the practice management system can’t match payments with their originating charges, the practice should calculate this using aged data, typically from six months back, to ensure a majority of the claims used for calculating have had enough time to clear.
An overall net collection rate of 95-99% or greater is average performance. If the net collection rate is less than 95% then it can be an indicator of poor performance.
Perhaps one of the most important KPIs to monitor is the percent of collections completed on the day of service (which should ideally be around 90%).
Collecting co-pays, deductibles, service fees, and other patient payments at the time of the visit helps to minimize past due payments. Instituting a firm financial policy and communicating each patient's financial obligations before the visit can assist your practice with increasing the percent of collections completed on the day of service.
The denial rate is the percentage of claims denied by payers. A low number is desired as it represents a practice’s cash flow and the staff needed to maintain that cash flow. Clean, paid claims do not require the attention that denied claims do by staff members.
How to calculate: Using a specific period of time—the last quarter, for example—total the dollar amount of claims denied by payers. The sum is then divided by the total dollar amount of claims submitted by the practice during that period of time. Practices may want to use charge line items denied divided by total charge line items submitted.
An average denial rate is typically between 5-10%. Denial greater than 10% can be an indication of poor performance.
Today's healthcare leaders understand that they must consider outsourcing the revenue cycle management to reduce spending and focus on value-based care initiatives. Some assume that the cost of outsourcing the billing operations would be more expensive than doing the billing in-house. After all, outsource fees typically range from 3% to 8% of net collections.
However, a report conducted by National Healthcare Exchange Services reports that physician practices are spending as much as 14% of their total collections to ensure accurate reimbursement from health insurers.
As medical practices consider outsourcing the medical billing functions verses performing the process internally, the related cost of each option should be considered and analyzed closely. This analysis involves more than simply comparing the billing services fees to the salary of internal billing staff. A proper in-house vs outsourced medical billing analysis can illustrate a substantial price difference between the two options when done correctly.
When evaluating the cost of performing billing and reimbursement functions internally, a practice should quantify the following items:
This cost should include the pay of all individuals involved in the medical billing and reimbursement functions.
Benefits like vacation, health insurance, retirement plans, social security, and unemployment can add up. The cost of staff benefits may equal as much as 20% to 30% of the salary and wage total.
Compliance, medical coding and reimbursement rules and regulations are continuously changing and may change substantially from year to year. On top of that, your medical billing staff may also need to obtain training on new quality payment programs like the Merit-based Incentive Payment System. It is necessary for billing staff to stay current on industry developments, not only for compliance issues, but also to protect your bottom line.
Space currently occupied by internal billing staff could be eliminated or used as revenue producing space such as an extra exam room.
The cost of losing an employee can range from tens of thousands of dollars to 1.5 to 2.0x the employee’s annual salary according to Josh Bersin of Deloitte. When calculating the specific cost of losing an employee at your medical practice, consider the cost of hiring, onboarding and training, ongoing learning and development, and the associated costs during the time of the unfilled role including recruitment and productivity costs. For the sake of this internal vs outsourced medical billing analysis, we will assume the estimated cost associated with the staffing process equals $10,000 per occurrence.
Physicians often note that the handling of staff and personnel issues can be one of the least desirable duties of a medical practice. The cost of time required to manage billing personnel and related issues should be considered. If the function is performed by the physician, opportunity costs include lost patient care revenue.
Medical practices not currently sending the majority of their claims electronically, will be in the very near future.
Collecting patient payments is becoming increasingly more difficult and is a major pain point for practices. In fact, average practices spend a total of $2.41 on materials and admin costs associated with sending paper statements which includes printing, postage, and processing.
The costs associated with Electronic Health Record (EHR) software systems can add up. When transitioning to an integrated EHR software there are a number of costs to consider and whether these costs are indirect or direct costs. Direct costs will include things like the EHR software licenses, upgrades, support, annual maintenance, and integrations. Indirect costs of transitioning to an EHR must be considered as well. The indirect cost of switching EHRs may vary but typically this cost will be related to productivity losses during and after EHR go-live. Fully implementing an EHR into practice workflows is estimated to take nearly 134 hours for the average EHR. When implementing an EHR software, anticipate a learning curve not only during initial go-live but as new versions and features are released over time. Without continuous EHR optimization and an EHR strategy to improve adoption, practices risk incurring even more unnecessary costs due to inefficiencies and underutilization of EHR software.
Medical billing staff will require computers, phones, desks, chairs, faxes, copiers and other standard office equipment that must be taken into consideration.
Standard office supplies can also get expensive with a centralized billing office. Office supplies such as paper, pens, postage, envelopes, copy, fax, and printer supplies are all utilized during the medical billing process.
Additional phone lines and/or web conferencing user licenses can add to in-house billing costs.
An internal billing process may not provide for the necessary separation of revenue functions that assist in preventing and early detection of theft and embezzlement. Your practice may be at an increased risk if only one person handles the cash and books.
According to the Centers for Medicare and Medicaid Services (CMS), 30 percent of claims are denied or ignored on the first submission while 60 percent of those claims are never resubmitted. This means a medical practice will not be paid for those services. On top of this missed revenue, 90% of denials are avoidable. Whether you keep your billing in-house or outsource it, there are a number of ways to increase practice revenue both proactively and reactively. A medical billing department or outsourced billing service should be both proactive and reactive in streamlining the claims process and finding ways to prevent and appeal claim denials.
In the following scenario, the medical practice “Best Medical”, with 3 providers, collects $1,200,000 per year and needs two billing clerks to handle this level of activity. Each billing clerk earns an average annual salary of $36,000. The billing clerks occupy an area that is 150 square feet of space and the space rents for $17 per square foot. Each of the clerks attends a billing seminar every other year with each participating in a quarterly online webinar. The average length of employment for each clerk is 2 years. The staff is top-notch and much better than the industry average due to the fact that they make no medical billing errors. Furthermore, the top notch staff will require very little supervision and the practice experiences no theft or embezzlement. The typical cost associated with this first rate internal billing function may include the following:
|
Salary and Wages |
$72,000 |
|
Employee Benefits |
$18,000 |
|
Training Costs |
$2,500 |
|
Real Estate & Occupancy |
$3,000 |
|
Staffing Turnover Costs |
$5,000 |
|
Equipment Cost and Office Supplies |
$1,300 |
|
Communication Costs |
$2,000 |
|
EDI Costs |
$1,800 |
|
Statement Costs |
$2,400 |
|
Technology Costs |
$13,200 |
|
Total Internal Cost of Billing Functions |
$121,200 |
|
Cost as a Percentage of Collections |
10.1% |
| Annual Expenses - Medical Billing Functions | |
|---|---|
The above example assumes that the internal billing department does not make any mistakes or errors. This scenario is unlikely as studies indicate that the average internal billing department makes errors resulting in losses of 25%-30% of practice income. Using the same assumptions as the above case, assume that the internal billing department of medical practice “Above Average Medical” is fairly competent (instead of perfect) and only makes errors that result in lost revenue of 5% to the practice. As illustrated below, even a slight medical billing error rate can substantially increase the cost of the internal billing function:
| Annual Expenses - Medical Billing Functions | |
|---|---|
|
Total Internal Cost of Billing Functions as stated above |
$121,200 |
|
Lost Revenue as Result of 5% Errors |
$60,000 |
|
Total Internal Cost of Billing Functions |
$181,200 |
|
Cost as a Percentage of Collections |
15.01% |
Now that you’ve analyzed the costs associated with in-house medical billing vs outsourced medical billing, it’s time to consider how you might select a revenue cycle management service.
Check out our document comparing Full vs Lite RCM Solutions.
The global healthcare revenue cycle management outsourcing market is slated to increase considerably, with its valuation rising from just $11.7 billion in 2017 to $23 billion by the end of 2023, a new market report shows. With the outsourcing market growing, your options for a revenue cycle management partner can seem endless.
But more doesn’t always mean better. While outsourcing is on the rise, finding the right company to partner with for revenue cycle management services can be time consuming and complicated. The right billing service can positively affect cash flow by decreasing the cost associated with the revenue cycle functions but when the wrong billing service is chosen, long term contracts and cash flow disruptions can become detrimental.
One of the key benefits of a centralized billing office is the ease of communication. Having the medical coder down the hall from the physician can be extremely valuable but when you’re considering outsourcing, how does this communication between the medical coder and provider take place?
Aside from provider to coder communication, outsourcing can make resources you might have traditionally had access to down the hall less available. But outsourcing your medical billing doesn’t have to mean less communication just because of location. Modern day technology is making it easier for teams to communicate conveniently anywhere, anytime.
Understand upfront how your staff will communicate with the billing service by asking questions like:
How do I get in touch with our account representative?
What is the typical turnaround time if I submit a support case?
When will we meet to review reports and account performance?
How will providers communicate with medical coders?
