Click above for a quick overview
Table of Contents
I. Navigating Financial Headwinds and Policy Shifts: The 2026 Regulatory & Reimbursement Landscape
Medicare Physician Fee Schedule 2026: A Welcome But Complicated Update
What is the CMS Efficiency Adjustment and How Does It Impact Procedural Specialties?
Practice Expense Methodology and Site-of-Service Differentials
CPT 2026 Code Set Updates: AI Billing Codes, Remote Monitoring, and Revascularization
Behavioral Health Integration and Clinical Social Worker Enhancements
How Does the One Big Beautiful Bill Act Affect Medicaid Funding for Medical Practices?
Telehealth Policy: Two-Year Extension Brings Stability, Not Permanence
II. Revenue Cycle Management & Financial Operations: Optimizing for Resilience
The Payer-Provider AI Dynamic: A New Revenue Landscape
The Shift Toward Strategic Outsourcing and Nearshoring
The Evolving Patient Financial Experience
III. Technology Transformation: AI Governance Takes Center Stage
AI Adoption Surges Past the Tipping Point
Shadow AI and Governance: The Critical Challenge of 2026
IV. Core Operational Imperatives: Staffing, Costs, and Patient Focus
Staffing Challenges: From Crisis Mode to Strategic Workforce Redesign
Administrative Stability as a Core Clinical Metric
Cost Reduction and Efficiency: The Imperative Intensifies
Value-Based Care Evolution: The 10-Year LEAD Model
V. Conclusions: Navigating Pressure and Opportunity in 2026

Welcome to “Medical Practice Industry Information You Should Know,” your regular update from Revele. The landscape for medical practices in 2026 is defined by a paradox: a long-awaited uptick in Medicare physician payment arrives alongside sweeping policy changes that threaten to erode those gains. From the first positive Medicare conversion factor update in years—offset by a controversial new efficiency adjustment and a fundamental restructuring of practice expense methodology—to historic Medicaid funding cuts under the One Big Beautiful Bill Act, practices face a complex and rapidly evolving environment.
Add in an impending HIPAA Security Rule overhaul, the explosive mainstreaming of AI across clinical and administrative workflows, new CPT codes that create direct reimbursement pathways for AI-driven clinical services, the emergence of mandatory specialty risk models, and persistent workforce challenges, and the imperative to stay informed has never been greater. This post dives into the key developments shaping the business of medicine today, offering insights to help your practice thrive in the year ahead.
Key Takeaways — Spring 2026
Last Updated: March 10, 2026
- The 2026 Medicare conversion factor rises 3.26% to $33.4009, the first increase in six years, driven by the One Big Beautiful Bill Act’s temporary 2.5% update.
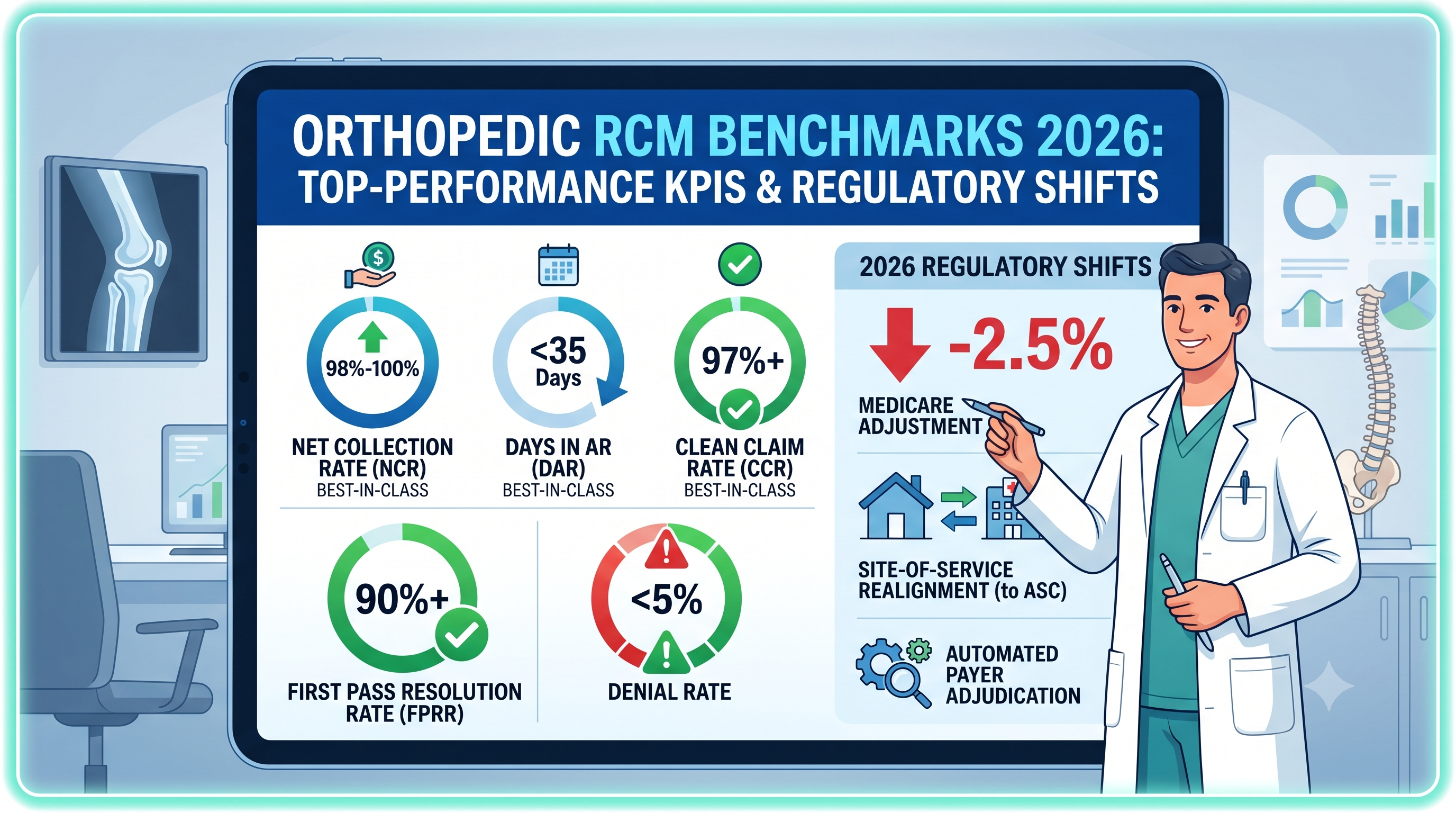
- A new -2.5% CMS efficiency adjustment to work RVUs disproportionately impacts procedural specialties, potentially neutralizing the payment increase.
- The One Big Beautiful Bill Act cuts federal Medicaid spending by $911B–$1T over 10 years, with enhanced FMAP sunset, eligibility narrowing, and 6-month redeterminations taking effect in 2026.
- A major HIPAA Security Rule overhaul mandates MFA, encryption, and penetration testing, with compliance expected by late 2026 or early 2027.
- New AI-specific CPT codes (including 75577, 0992T, and 0993T) create direct reimbursement pathways for augmented-intelligence clinical services.
- 68% of physicians now use AI tools in practice (up from 38% in 2023), and 53% of healthcare organizations have adopted agentic AI workflows.
- Medicare telehealth flexibilities extended through December 31, 2027, providing a stable two-year policy runway.
- The mandatory Ambulatory Specialty Model (ASM) begins in 2027, with payment adjustments of -9% to +9% for targeted specialties in selected CBSAs.
MGMA polling reveals how medical group executives are prioritizing their strategic budgets for 2026: 37% of new dollars are directed toward workforce stabilization, 30% toward health information technology and cybersecurity, 12% toward revenue cycle automation, and 12% toward expanding patient access channels. These allocations underscore an industry consensus that traditional, labor-intensive practice management models are no longer viable in an environment of constrained reimbursement and escalating costs.
I. Navigating Financial Headwinds and Policy Shifts: The 2026 Regulatory & Reimbursement Landscape
Medical practices in 2026 operate within a regulatory environment that simultaneously offers relief and imposes new constraints. After several consecutive years of overall reductions in the conversion factor, Medicare physician payments are set to rise in 2026 compared with 2025, though the details reveal a more nuanced picture. Concurrently, sweeping federal legislation is reshaping the Medicaid program, cybersecurity mandates are tightening, new coding frameworks create AI reimbursement pathways, and telehealth policy has narrowly avoided collapse.
Medicare Physician Fee Schedule 2026: A Welcome But Complicated Update
The Centers for Medicare & Medicaid Services (CMS) finalized the Calendar Year 2026 Medicare Physician Fee Schedule (PFS) on October 31, 2025, delivering the first meaningful payment increase in years. For the first time under MACRA, CMS is implementing two separate conversion factors based on participation in Advanced Alternative Payment Models (APMs). The non-qualifying APM conversion factor rises to $33.4009 (a 3.26% increase from 2025), while the qualifying APM conversion factor reaches $33.5675 (a 3.77% increase).
Much of this increase is attributable to the temporary 2.5% update Congress passed as part of the One Big Beautiful Bill Act (OBBBA H.R. 1), signed into law on July 4, 2025. While this represents a welcome reversal after five consecutive years of conversion factor cuts, the 2.5% update is a one-time adjustment for 2026 only—it does not create a permanent, inflation-adjusted payment mechanism. Earlier proposals that would have tied Medicare updates directly to the Medicare Economic Index (MEI) were stripped from the final legislation, ensuring that, in real economic terms, Medicare reimbursements continue to erode against the rising costs of clinical labor, rent, and medical supplies.
The remaining increase in the conversion factor stems from small, permanent MACRA baseline updates (0.75% for APM-qualifying participants and 0.25% for all others) and a positive 0.49% budget-neutrality adjustment. The AMA continues to advocate for permanent baseline updates tied to MEI growth, and MedPAC has warned that the widening gap between payments and costs could drive physicians to reduce their Medicare patient panels, exit Medicare entirely, or consolidate with hospitals—all outcomes that would reduce beneficiaries' access to care.
What Is the CMS Efficiency Adjustment and How Does It Impact Procedural Specialties?
The most controversial element of the 2026 PFS is the introduction of a negative 2.5% efficiency adjustment applied to the work RVUs and corresponding intraservice physician time for nearly all non-time-based services. CMS argues that current RVU valuations do not account for efficiencies gained through technological advancement, improved instrumentation, and optimized clinical protocols. The adjustment exempts time-based codes, including E/M services, behavioral health, care management, telehealth-listed services, and maternity codes, as well as codes newly created for 2026.
The impact falls disproportionately on procedural and diagnostic specialties. The AMA’s analysis found that 80% of infectious disease physicians face cuts of 5% or more. CMS has signaled it will apply the efficiency adjustment on a recurring three-year cycle moving forward, subject to future rulemaking. However, CMS provided a critical safe harbor by agreeing to exempt any newly created Category I CPT codes initially assigned a value for 2026 from this punitive adjustment. For multi-specialty groups, orthopedic practices, and ambulatory surgery centers, the 2.5% aggregate conversion factor increase provided by H.R. 1 may be entirely neutralized—or surpassed—by this compounding RVU suppression on their core procedural service lines.
Practice Expense Methodology and Site-of-Service Differentials
Recognizing the macro-trend toward physician practice consolidation into hospital employment models, CMS has finalized a fundamental revision to indirect Practice Expense (PE) RVU allocations by site of service. For services performed in hospital settings, the portion of indirect PE allocated based on work RVUs is reduced by 50% starting in 2026, on the premise that hospitals now bear those overhead costs.
The net effect is significant: CMS estimates that facility-based physician payments will drop by approximately 7% overall, while payments for services in independent office-based settings will rise by roughly 4%. Individual physicians providing a high volume of facility-based services could see substantially larger cuts. AMA President Bobby Mukkamala, MD, expressed concern that these changes could make it harder for independent practices to remain viable, potentially accelerating consolidation.
For practice administrators, this rebalancing creates a distinct financial advantage for autonomous practices that can effectively manage their direct overhead costs. Practices evaluating real estate decisions, considering transitioning from hospital-based to independent ambulatory settings, or negotiating hospital joint ventures must incorporate these updated site-of-service differentials into their financial models. The profitability delta between independent and facility-based care delivery will continue to widen in 2026.
CPT 2026 Code Set Updates: AI Billing Codes, Remote Monitoring, and Revascularization
The AMA’s 2026 Current Procedural Terminology (CPT) code set release reflects an industry aggressively pivoting toward digital health, precision analytics, and minimally invasive interventions. The updated set includes 418 total structural changes: 288 new codes, 84 deletions, and 46 revisions. Category III codes—designating emerging medical technologies—account for more than 27% of newly established codes, underscoring the rapid pace of clinical innovation that practices must absorb into their billing infrastructure.
AI-Specific Billing Codes: The 2026 code set marks a watershed moment by establishing independent reimbursement pathways for augmented intelligence (AI) clinical services. These codes differentiate between software that organizes data and advanced algorithmic systems that independently assess, quantify, and detect clinically relevant pathologies. Notable additions include codes for noninvasive coronary atherosclerotic plaque quantification via AI-enhanced CT angiography (which graduated to a permanent Category I code 75577), and new Category III tracking codes for cardiac risk assessment via algorithmic analysis of perivascular fat (0992T and 0993T), acoustic and ECG algorithmic detection of reduced ejection fraction and asymptomatic atrial fibrillation, and burn wound multispectral imaging classification. These codes transform AI from an uncompensated overhead expense into a direct revenue-generating service line, fundamentally altering ROI calculations for medical groups considering AI acquisitions.
Short-Duration Remote Patient Monitoring: Evidence that continuous 30-day RPM is not universally required has led to new codes addressing lower utilization thresholds, including 99445 to capture device supply and transmission lasting 2–15 days, and 99470 to capture 10-19 minutes of RPM clinical treatment management time. Additionally, a new, granular RPM treatment management code (99470) allows billing for 10 to 19 minutes of care, capturing clinical work that previously went uncompensated under the strict 20-minute minimum of legacy code 99457. This flexibility allows practices to deploy RPM more surgically for post-operative surveillance and acute medication titration without triggering the 16-day minimum data transmission requirements of legacy codes.
Revascularization Code Overhaul: The most expansive structural reorganization in the surgical domain is the comprehensive rebuild of the lower extremity revascularization section, introducing 46 new territory-based codes (37254–37299) organized across four vascular regions with gradations for straightforward versus complex lesion morphologies. Vascular surgery and interventional practices will need intensive coder retraining and EHR template updates to prevent denial cascades.
Laboratory and Pathology Expansion: An extensive expansion of Proprietary Laboratory Analyses (PLA) codes reflects the rapid integration of genomic sequencing, targeted oncology biomarkers, and advanced infectious disease panels into ambulatory care. Practices overseeing clinical labs or oncology services must update their Charge Description Masters to capture these highly specific codes.
Behavioral Health Integration and Clinical Social Worker Enhancements
Responding to a worsening national mental health crisis and acute shortages of psychiatric personnel, CMS has implemented aggressive reimbursement strategies to bolster behavioral health access within the Medicare population. A cornerstone of this effort is the creation of optional add-on G-codes for Advanced Primary Care Management (APCM) services. When an APCM base code is billed in a given month, new G-codes can be reported to account for behavioral health integration (BHI) or psychiatric Collaborative Care Model (CoCM) services. This bundled approach reduces administrative friction and heavily incentivizes primary care practices to embed behavioral health coordinators directly into clinical workflows.
Despite aggressive lobbying from mental health advocates to elevate Clinical Social Worker (CSW) reimbursement to 85% of the MPFS—which would have created parity with allied professionals like physical therapists—CMS opted in the final rule to maintain CSW, LPC, and MFT reimbursements at the historical 75% benchmark. Furthermore, CMS declined requests to bypass Consolidated Billing rules, meaning independent CSWs remain prohibited from billing Medicare Part B for mental health services rendered to beneficiaries currently enrolled in a Part A-covered skilled nursing facility (SNF) stay.
For practices with behavioral health service lines or those considering integration, these changes create meaningful new revenue opportunities. The combined effect of APCM behavioral health add-ons and CSW payment parity makes embedded behavioral health models significantly more financially viable in 2026.
How Does the One Big Beautiful Bill Act Affect Medicaid Funding for Medical Practices?
The One Big Beautiful Bill Act (OBBBA), signed on July 4, 2025, represents the most significant restructuring of Medicaid in decades. The Congressional Budget Office estimates the law will reduce federal Medicaid spending by approximately $911 billion to $1 trillion over ten years. While the most dramatic changes phase in over several years, key provisions affecting practices in 2026 include:
- Enhanced FMAP Sunset (January 1, 2026): Phases down certain temporary enhanced FMAP provisions beginning January 1, 2026, increasing state financing responsibility for some populations, which may prompt eligibility or benefit changes in some states.
- Eligibility Narrowing for Non-Citizens (October 1, 2026): Medicaid eligibility restricted to lawful permanent residents with at least five years of U.S. residency and certain other defined categories.
- Provider Tax Freeze (Effective Immediately): States prohibited from establishing new provider taxes or increasing existing ones—a critical financing mechanism many states relied on.
- Work Requirements (January 1, 2027) & 6-Month Redeterminations (December 31, 2026): Able-bodied adult recipients must document 80+ hours/month of work, training, or community service. Six-month eligibility redeterminations replace annual reviews.
- Elimination of “Addressable” Standards: All Security Rule specifications become mandatory with limited exceptions. The flexibility to document why a control was not implemented will be removed.
- Mandatory MFA: Required for all systems accessing ePHI, both onsite and remote.
- Encryption at Rest and in Transit: All ePHI must be encrypted in accordance with NIST standards.
- Regular Technical Testing: Vulnerability scanning every six months; penetration testing annually.
- Technology Asset Inventories and Network Segmentation: Comprehensive inventories, network maps, and segmentation of ePHI systems are required.
- BA Verification and Access Controls: Annual verification of business associate security measures; system access revocation within one hour of termination.
- Technology and Automation: AI across RCM, documentation, scheduling, eligibility verification, and patient communication.
- Workflow Optimization: Dashboard analytics tracking acquisition costs, treatment profitability, and provider productivity to identify hidden optimization opportunities.
- Supply Chain and Overhead: Vendor consolidation, GPO utilization, inventory controls, and energy efficiency measures.
- Care Delivery Adjustments: Shifting appropriate care to lower-cost settings, leveraging telehealth and remote patient monitoring, and emphasizing preventive care.
- Strategic Outsourcing: Engaging specialized partners for RCM, IT, and coding where external scale delivers better cost-performance ratios.
- Heart Failure: Mandated for general cardiology physicians.
- Low Back Pain: Mandated for orthopedic surgery, neurosurgery, anesthesiology, physical medicine and rehabilitation, and interventional pain management.
- Invest in AI strategically: Focus on high-ROI applications—ambient documentation, denial prediction, prior authorization automation, and the new AI-specific CPT codes—while establishing governance to manage shadow AI risk.
- Model the financial impact of 2026 changes: The efficiency adjustment, site-of-service differentials, and Medicaid cuts will affect every practice differently. Specialty- and payer-mix-specific financial modeling is essential.
- Prepare for mandatory VBC: Cardiology, orthopedic, and neurosurgery practices in targeted CBSAs must begin ASM preparation immediately. All practices should evaluate LEAD readiness.
- Get ahead of HIPAA compliance: Begin security assessments, implement MFA, verify BA compliance, and diversify clearinghouse vendors.
- Treat workforce as a strategic priority: Invest in technology that reduces administrative burden, redesign care teams, elevate administrative stability as a clinical metric, and build cultures of recognition and support.
- Optimize the revenue cycle with urgency: AI-powered RCM, strategic outsourcing, proactive denial management, and front-end patient financial engagement are essential survival strategies.
HIPAA Security Rule Overhaul: Mandatory Cybersecurity Standards on the Horizon
The proposed update to the HIPAA Security Rule, published January 6, 2025, represents the most substantial overhaul of healthcare cybersecurity requirements in over a decade. Regulators aim to finalize the rule by mid-2026, with compliance deadlines likely falling by late 2026 or early 2027. The changes will fundamentally shift HIPAA compliance from policy documentation to measurable, enforceable cybersecurity programs:
OCR levied more than $6.6 million in HIPAA fines in 2025, with penalties ranging from $80,000 to $3 million. The third phase of HIPAA compliance audits is now underway, initially targeting 50 covered entities. Practices should not wait for the final rule—begin security risk assessments, implement MFA, verify BA compliance, and budget for the investments the final rule will require. The Change Healthcare attack underscored the imperative of vendor diversification: practices are actively restructuring clearinghouse architectures to build mandatory redundancy, ensuring financial operations remain functional during future cyber disruptions.
Telehealth Policy: Two-Year Extension Brings Stability, Not Permanence
After a tumultuous 2025 that included a 43-day lapse in Medicare telehealth coverage during the government shutdown—with one analysis estimating a 24% national drop in telehealth visits —Congress delivered meaningful relief. The Consolidated Appropriations Act of 2026 extended most Medicare telehealth flexibilities through December 31, 2027, providing the most stable policy footing since the pandemic era.
Through the end of 2027, Medicare patients can receive non-behavioral telehealth services in their homes with no geographic restrictions; all eligible practitioners (including PTs, OTs, SLPs, and audiologists) can furnish telehealth services; audio-only visits remain reimbursable; and FQHCs/RHCs can serve as distant-site providers. CMS updated the Telehealth Originating Site Facility Fee (Q3014) to $31.85, a 2.7% increase.
Separately, the 2026 PFS final rule made several policies permanent: frequency limits on subsequent inpatient, nursing facility, and critical care telehealth consultations were removed; direct supervision was permanently redefined to allow virtual presence via audio-visual technology (with a strict prohibition on procedures carrying a 10- or 90-day global surgery indicator), and teaching physicians can permanently provide virtual supervision in all training settings. CMS also moved several behavioral health codes—including multiple-family group psychotherapy (90849), group behavioral counseling for obesity (G0473), and developmental/neuropsychological testing—onto the permanent Medicare Telehealth Services list.
However, the AMA and other organizations continue pushing for permanent legislation. Beginning January 1, 2028, without further Congressional action, strict pre-pandemic limitations will resume: patients must travel to designated medical facilities in rural areas, therapists lose telehealth authorization, and home-based originating sites will end for non-behavioral services.

II. Revenue Cycle Management & Financial Operations: Optimizing for Resilience
The revenue cycle landscape in 2026 is defined by an escalating technology-driven competition between payer utilization management algorithms and provider billing operations. Practice leaders are allocating approximately 12% of strategic budgets toward RCM optimization, signaling its critical role in organizational survival.
AI and Automation: From Pilot to Enterprise in RCM
The conversation around AI in revenue cycle management has shifted decisively from experimentation to enterprise deployment. AI applications now span the full revenue cycle—from real-time eligibility verification and prior authorization automation to predictive denial management, automated coding, intelligent AR prioritization, and appeals generation. “Agentic” AI tools—systems capable of autonomous decision-making and multi-step execution—are being deployed to manage benefits verification, eligibility checks, and the historically burdensome prior authorization process.
Case studies from early adopters report denial rate reductions of 30–50%, prior authorization times dropping from days to hours, clean claim rate gains of 15–30%, days in AR down 20–35%, and productivity increases of 25–40% for repetitive tasks, though results vary by organization. Leading industry analytics from 2026 reveal that 53% of healthcare organizations have adopted agentic AI or multi-agent workflows, marking a rapid strategic evolution from basic ambient scribing to fully autonomous execution of administrative and clinical tasks.
Some industry analyses project that broad adoption of RCM and administrative automation could eventually yield up to roughly 360 billion dollars in annual savings across the healthcare system. MGMA data indicates coding support and payer analytics rank among the highest RCM investment priorities for 2026. The critical success factor remains seamless integration with existing PM and EHR systems. Practices evaluating AI-RCM vendors should rigorously assess integration depth, data security, and demonstrated outcomes in comparable environments.
The Payer-Provider AI Dynamic: A New Revenue Landscape
A notable development in 2026 is the emergence of what Bessemer Venture Partners calls the “payer-provider AI arms race.” As providers have become more effective at capturing appropriate reimbursement through AI-powered coding, documentation, and claims management, medical loss ratios on the payer side have crept upward. This is not fraud or overutilization—it reflects providers getting better at securing legitimate reimbursement.
In response, payers are accelerating their own AI adoption for payment integrity, claims review automation, prior authorization, fraud detection, and utilization management. This creates a dynamic in which both sides leverage increasingly sophisticated AI, and practices that fail to keep pace risk falling behind in an environment where payers deploy more advanced audit and review algorithms. AI-powered RCM is no longer a competitive advantage; it is becoming table stakes.
The Shift Toward Strategic Outsourcing and Nearshoring
Staffing volatility within specialized billing roles has accelerated the transition toward strategic outsourcing. The outsourced RCM market is forecasted to nearly double within a four-year horizon, with up to 70% of hospitals, health systems, and larger medical groups planning to expand third-party engagements. A dominant trend for 2026 is the rapid expansion of nearshore outsourcing, primarily leveraging talent pools in Latin America to enable same-time-zone collaboration on high-touch, judgment-intensive processes such as complex clinical coding and denial appeals.
Financial analyses suggest that comprehensive end-to-end outsourced RCM and virtual staffing models can deliver operational cost savings of 30–40% compared to maintaining fully burdened in-house billing departments. By shifting RCM from a fixed internal cost to a variable outsourced expense tied to collections, practices can insulate margins from local labor market fluctuations. The integration of virtual medical assistants and dedicated remote billing specialists provides scalable expertise without geographic constraints.
The Evolving Patient Financial Experience
The financial relationship between practices and patients continues to evolve, shaped by rising cost-sharing through high-deductible health plans, potential Medicaid coverage losses under OBBBA, and the March 2025 CFPB rule that broadly restricts medical debt in credit reporting. With the credit-reporting lever effectively eliminated, practices must pivot toward front-end financial processes: robust pre-service financial clearance, accurate AI-powered eligibility verification, transparent pre-service cost estimates, clear communication of financial responsibility, and convenient digital payment options.
Organizations are investing in digital front doors and AI-enabled payment tools to capture patient responsibility upfront, prior to the clinical encounter. This involves automated out-of-pocket estimates at scheduling, flexible mobile-app-based payment plans, and consumer-centric billing experiences. Practices that treat the patient's financial experience with the same focus as retail transactions reduce friction, increase point-of-service collections, and protect their bottom line against post-adjudication default.

III. Technology Transformation: AI Governance Takes Center Stage
Health information technology commands an impressive 30% share of new budget allocations for medical groups in 2026. The nature of this investment has shifted from foundational EHR adoption to advanced computational workflows, robust security infrastructure, and—critically—governance frameworks to manage the risks of rapid AI deployment.
AI Adoption Surges Past the Tipping Point
AI adoption in healthcare has crossed a critical threshold. Recent data indicate a rapid surge in the adoption of artificial intelligence by healthcare providers, with approximately 66% to 68% of physicians reporting the use of AI tools in their practice as of early 2025. This represents a significant increase from 38% in 2023, showcasing a rapid, widespread integration into clinical workflows. A Menlo Ventures analysis found that healthcare is adopting AI at twice the rate of the broader economy. AI tools have overtaken EHR usability as the top technology priority for medical practice leaders.
The FDA cleared 295 AI-enabled diagnostic tools in 2025 alone. Per a survey by Healthcare Dive and Microsoft, Planned adoption of clinical documentation AI is projected to increase by 320% in the near term. Meanwhile, HHS’s Office of the Assistant Secretary for Technology Policy issued a Request for Information in December 2025 on driving clinical AI adoption, drawing proposals from Epic, Oracle, Abridge, and others. The Trump administration has signaled a deregulatory posture toward AI, pursuing a national framework and emphasizing a lighter‑touch, innovation‑oriented federal approach to AI governance, even as states advance their own AI laws.
From Ambient to Agentic AI: The Strategic Frontier
In 2025, 71% of practices reported adding or expanding AI specifically for patient visits, primarily utilizing ambient listening technologies that draft clinical notes in real time. Some studies of ambient documentation tools report large reductions in documentation workload—approaching 80% in certain data‑heavy specialties—and 1–2 hours of time savings per day for participating physicians.
However, the strategic frontier for 2026 involves the transition from ambient to “agentic” AI. While ambient AI acts as a passive, efficient scribe, agentic AI operates as an active, autonomous digital proxy. These systems can autonomously interpret a complex lab result, draft a contextually appropriate patient communication, queue the necessary follow-up appointment, and generate the corresponding prior authorization request—all requiring only a single confirmatory click from the attending provider.
The prioritization of agentic tools has surpassed even basic EHR usability enhancements, as practice executives recognize their capacity to solve clinician burnout by automating multi-step administrative workflows. The NVIDIA survey found 47% of healthcare organizations are already using or assessing agentic AI. Combined with the new CPT AI billing codes that create direct reimbursement pathways, the ROI equation for enterprise AI investments is shifting from cost avoidance to revenue generation.
Shadow AI and Governance: The Critical Challenge of 2026
As AI adoption accelerates, “shadow AI”—generative AI tools used in healthcare outside institutional oversight—has emerged as a critical concern. Health system leadership is playing catch-up to clinicians who have rapidly adopted GenAI on their own, often without vetting, validation, or security review. Users may encounter responses that appear authoritative but are clinically invalid, and there is growing concern about “clinical deskilling” due to over-reliance on AI for diagnosis and treatment planning.
Industry experts are calling 2026 “the year of governance.” Practices should ensure that any AI tools used in clinical or administrative settings are purpose-built for healthcare, trained on validated clinical evidence, transparent in sourcing and reasoning, HIPAA-compliant, and formally approved through an organizational governance process.
The regulatory landscape is fragmented: while the federal government pursues deregulation, all 50 states introduced AI legislation during the last session, and nearly 40 adopted measures. Some states now require providers to disclose to patients the use of AI. Practices should monitor both federal and state developments and work with legal counsel to ensure compliance.
IV. Core Operational Imperatives: Staffing, Costs, and Patient Focus
Despite rapid technological advancement, healthcare remains a profoundly human endeavor. The most acute vulnerabilities facing practice administrators in 2026 revolve around the acquisition, retention, and optimal utilization of human capital. Workforce stabilization has emerged not merely as an HR objective but as a defining clinical metric.
Staffing Challenges: From Crisis Mode to Strategic Workforce Redesign
The healthcare workforce enters 2026 under mounting strain. The AHA projects a shortage of up to 3.2 million healthcare workers by 2026. An Indeed survey found that two in five healthcare workers report that their jobs feel unsustainable. Workers report being short-staffed 43% of the time, and 80% say existing well-being programs are ineffective because they fail to address root causes.
While aggregate turnover has stabilized slightly, MGMA data reveals a critical vulnerability at the point of care: medical assistants and front-office staff continue to experience extraordinarily high churn, driven by administrative burden, patient incivility, and aggressive wage competition from retail and hospitality sectors. Broad psychological polling indicates that 77% of workers report increased work-related stress, while specific MGMA polling found that 36% of practice leaders say they never disconnect from work. A JAMA Internal Medicine study found nearly half of physicians work with incompletely staffed teams more than 25% of the time—and are twice as likely to report burnout.
Strategies gaining traction include market-adjusted wage floors, career-laddering programs with employer-funded certifications, expanded APP and locum tenens utilization, AI tools that directly reduce administrative burden, and automated self-check-in kiosks and AI-driven call centers that remove low-value tasks from the front desk. Crucially, 70% of physicians now view organizational culture and operational support as on par with compensation in retention decisions.
Administrative Stability as a Core Clinical Metric
A paradigm shift is underway: the most sophisticated health organizations now recognize that consistent, highly trained administrative teams are as integral to clinical outcomes as the practitioners themselves. Workforce stability is being integrated into core operational performance dashboards, with analytical models correlating staff retention rates directly to revenue realization, clinical error reduction, and patient satisfaction.
Organizations that fail to treat their administrative workforce as a strategic clinical asset risk cascading failures in care continuity, delayed diagnostic follow-ups, and compromised quality reporting. Leading practices are investing in cross-training, formal apprenticeship partnerships with local educational institutions, and technology that elevates administrative roles from transactional clerks to care coordinators.
Cost Reduction and Efficiency: The Imperative Intensifies
The convergence of a still-inadequate Medicare payment update, rising operational costs (commercial medical costs projected to jump 8.5% in 2026), looming Medicaid revenue losses, and persistent growth in staffing expenses makes efficiency more critical than ever. Practices are deploying strategies across multiple domains:
Value-Based Care Evolution: The 10-Year LEAD Model
As the ACO REACH model concludes its final performance year in 2026, CMS is preparing its successor: the Long-term Enhanced ACO Design (LEAD) Model, scheduled to run from January 1, 2027, through December 31, 2036. With the Request for Applications opening in Spring 2026, forward-looking practices must evaluate their readiness now. The Medicare Shared Savings Program currently has 477 ACOs serving 11.2 million beneficiaries, and CMS data indicates VBC arrangements are expected to cover 45% of Medicare beneficiaries by the end of 2026.
LEAD introduces revolutionary design elements engineered to solve the historical “ratchet effect” that penalized successful ACOs with ever-lower benchmarks. The most significant innovation is a 10-year performance period with no benchmark rebasing, providing the long-term ROI certainty that independent and rural practices need to invest in population health infrastructure. LEAD offers two risk tracks: a Professional Risk Option (capping shared savings and losses at 50%) and a Global Risk Option (allowing 100% risk/reward alongside capitated total cost-of-care payments).
Additional LEAD features include CMS-administered Risk Arrangements (CARA), which allow specialists to assume financial accountability for specific clinical episodes without assuming total population risk; beneficiary incentives, including Part B cost-sharing coverage and chronic disease prevention rewards; targeted mechanisms for high-needs populations; and Medicare-Medicaid integration frameworks. Quality measures will include CAHPS scores and new electronic clinical quality measures (eCQMs).
For practices considering VBC participation, LEAD’s 10-year horizon and structural innovations represent a fundamentally different value proposition than prior models. The combination of benchmark stability, flexible risk tracks, and specialist engagement pathways makes this the most compelling voluntary VBC opportunity in a decade.
Mandatory Risk Assumption: The Ambulatory Specialty Model (ASM)
While LEAD is voluntary, CMS is simultaneously deploying the Ambulatory Specialty Model (ASM)—a mandatory payment model that fundamentally alters the financial landscape for specific specialty physicians beginning in 2027. CMS will mandate participation for specialists in approximately 25% of randomly selected Core Based Statistical Areas (CBSAs), targeting two clinical cohorts with high Medicare expenditures and high care quality variability:
Any practitioner in selected CBSAs billing under the MPFS and attributed to 20 or more specific clinical episodes based on Episode-Based Cost Measures is legally required to participate. Critically, unlike MIPS, ASM requires assessment at the individual TIN/NPI level, thereby removing the protective averaging afforded by group-level reporting.
Participants receive a performance score (0–100) based on Quality (50% weight), Cost (50% weight), Improvement Activities (up to -20% penalty for non-compliance), and Promoting Interoperability (up to -10% penalty). During the first payment year (2029, based on a two-year lag from 2027 performance data), individual Part B reimbursements will be adjusted from -9% to +9%. The model operates as a zero-sum game: total positive adjustments cannot exceed total negative penalties, meaning specialists will be in direct financial competition with regional peers.
For cardiology, orthopedic, and neurosurgery practices in targeted CBSAs, preparation must begin immediately. The Improvement Activities requirement necessitates digital interoperability infrastructure and formal collaboration agreements with primary care networks. The combination of the PFS -2.5% efficiency adjustment and a potential -9% ASM penalty creates an environment in which operational inefficiency will quickly threaten the financial viability of specialty practices.

V. Conclusions: Navigating Pressure and Opportunity in 2026
The business environment for medical practices in 2026 is defined by a central tension: meaningful progress on several fronts alongside intensifying structural pressures. The first Medicare payment increase in years provides modest relief—but the efficiency adjustment, site-of-service rebalancing, and Medicaid cuts collectively create a far more complex financial picture than the headline conversion factor increase suggests.
Technology has moved from experimental to essential. AI ambient scribes are saving physicians hours per day. Agentic AI is automating multi-step workflows. New CPT codes are creating direct reimbursement pathways for AI-driven clinical services. And the revenue cycle is being transformed by AI tools that predict denials, automate authorizations, and optimize AR at scale. But the governance gap around clinical AI creates liability and patient safety risks that practices must address proactively.
The acceleration of advanced payment models—from the stabilizing 10-year horizons of the voluntary LEAD Model to the punitive, mandatory constraints of the Ambulatory Specialty Model—signals that total cost of care accountability is becoming the operational reality for both primary care and specialty providers.
For practice leaders, the strategic imperatives are clear:
The challenges detailed throughout this report—evolving reimbursement formulas, new coding frameworks, Medicaid restructuring, cybersecurity mandates, AI governance demands, mandatory specialty risk models, and persistent staffing pressures—create a landscape that rewards proactive, well-informed management. Partnering with a dedicated RCM and practice management expert like Revele can equip your practice with the technology, expertise, and strategic support needed to navigate these challenges, enhance financial performance, and empower your team to focus on what matters most: delivering exceptional patient care.

Frequently Asked Questions About 2026 Medical Practice Changes
What is the 2026 Medicare physician conversion factor?
The 2026 Medicare non-qualifying APM conversion factor is $33.4009, a 3.26% increase from 2025. The qualifying APM conversion factor is $33.5675, a 3.77% increase. Much of this increase comes from the temporary 2.5% update passed as part of the One Big Beautiful Bill Act (H.R. 1), signed July 4, 2025. This is a one-time adjustment for 2026 only and does not create a permanent inflation-adjusted payment mechanism.
What is the CMS efficiency adjustment in the 2026 Medicare Fee Schedule?
The CMS efficiency adjustment is a negative 2.5% reduction applied to work RVUs and intraservice physician time for nearly all non-time-based services in 2026. CMS argues this accounts for efficiencies from technological advancement and improved protocols. It exempts time-based codes including E/M services, behavioral health, care management, telehealth, and maternity codes. The adjustment disproportionately impacts procedural and diagnostic specialties.
How does the One Big Beautiful Bill Act affect Medicaid in 2026?
The One Big Beautiful Bill Act (OBBBA), signed July 4, 2025, reduces federal Medicaid spending by approximately $911 billion to $1 trillion over ten years. Key 2026 provisions include: enhanced FMAP sunset beginning January 1, 2026; Medicaid eligibility restricted to lawful permanent residents with 5+ years of U.S. residency starting October 1, 2026; a provider tax freeze effective immediately; and six-month eligibility redeterminations replacing annual reviews by December 31, 2026.
What are the new AI-specific CPT codes for 2026?
The 2026 CPT code set establishes the first independent reimbursement pathways for augmented intelligence clinical services. Notable additions include permanent Category I code 75577 for AI-enhanced CT coronary angiography plaque quantification, and new Category III tracking codes 0992T and 0993T for cardiac risk assessment via algorithmic perivascular fat analysis. These codes transform AI from an uncompensated overhead cost into a direct revenue-generating service line.
What is the Ambulatory Specialty Model (ASM) and which specialties are affected?
The Ambulatory Specialty Model (ASM) is a mandatory CMS payment model beginning in 2027 that targets cardiology, orthopedics, neurosurgery, and interventional pain management specialists in approximately 25% of randomly selected CBSAs. Performance is assessed at the individual TIN/NPI level with a 50/50 split between quality and cost. Part B reimbursements will be adjusted from -9% to +9% based on performance scores. It operates as a zero-sum model where total bonuses cannot exceed total penalties.
What are the proposed HIPAA Security Rule changes for 2026?
The proposed HIPAA Security Rule overhaul, published January 6, 2025, with finalization expected by mid-2026, eliminates the flexibility of addressable standards and makes all specifications mandatory. Key requirements include: mandatory multi-factor authentication (MFA), encryption of all ePHI at rest and in transit per NIST standards, vulnerability scanning every six months, annual penetration testing, comprehensive technology asset inventories, network segmentation, and annual business associate security verification.
What is the current state of Medicare telehealth policy in 2026?
The Consolidated Appropriations Act of 2026 extended most Medicare telehealth flexibilities through December 31, 2027. Through that date, Medicare patients can receive non-behavioral telehealth services at home with no geographic restrictions, audio-only visits remain reimbursable, and FQHCs/RHCs can serve as distant-site providers. Several policies were made permanent, including virtual direct supervision via audio-visual technology and removal of frequency limits on telehealth consultations.
What is the CMS LEAD Model for value-based care?
The Long-term Enhanced ACO Design (LEAD) Model is a voluntary CMS program running from January 1, 2027 through December 31, 2036. Its most significant innovation is a 10-year performance period with no benchmark rebasing. LEAD offers two risk tracks: a Professional Risk Option (50% cap on shared savings/losses) and a Global Risk Option (100% risk/reward with capitated payments). The Request for Applications opens in Spring 2026.
Works Cited
1. Calendar Year (CY) 2026 Medicare Physician Fee Schedule Final Rule (CMS-1832-F), CMS, October 31, 2025. https://www.cms.gov/newsroom/fact-sheets/calendar-year-cy-2026-medicare-physician-fee-schedule-final-rule-cms-1832-f
2. What to expect from the 2026 Medicare Physician Fee Schedule, AMA, December 11, 2025. https://www.ama-assn.org/practice-management/medicare-medicaid/what-expect-2026-medicare-physician-fee-schedule
3. CMS Releases 2026 Physician Fee Schedule Final Rule, American College of Cardiology, October 31, 2025. https://www.acc.org/Latest-in-Cardiology/Articles/2025/10/31/21/33/cms-releases-2026
4. CMS issues CY 2026 physician fee schedule final rule, AHA News, October 31, 2025. https://www.aha.org/news/headline/2025-10-31-cms-issues-cy-2026-physician-fee-schedule-final-rule
5. CMS Releases 2026 Medicare Physician Fee Schedule Final Rule, ASNC, October 31, 2025. https://www.asnc.org/news/cms-releases-2026-medicare-physician-fee-schedule-final-rule/
6. Physicians will see Medicare payments rise in 2026, AMA, July 21, 2025. https://www.ama-assn.org/practice-management/medicare-medicaid/physicians-will-see-medicare-payments-rise-2026
7. Medicare and Medicaid Programs; CY 2026 Payment Policies Under the Physician Fee Schedule, Federal Register, November 5, 2025. https://www.federalregister.gov/documents/2025/11/05/2025-19787/
8. CMS Releases CY 2026 Medicare Physician Fee Schedule Final Rule, Holland & Knight, November 2025. https://www.hklaw.com/en/insights/publications/2025/11/cms-releases-cy-2026-medicare-physician-fee-schedule-final-rule
9. What’s changing in Medicare for 2026—and why it matters, APA Services, 2025. https://www.apaservices.org/practice/reimbursement/government/medicare-final-rule-analysis
10. AMA releases CPT 2026 code set, AMA Press Release, 2025. https://www.ama-assn.org/press-center/ama-press-releases/ama-releases-cpt-2026-code-set
11. Understanding the CPT 2026 Code Set Updates, Wolters Kluwer, 2025. https://www.wolterskluwer.com/en/expert-insights/cpt-code-updates-2026
12. Physician Self-Referral Law – Annual Update to the List of CPT/HCPCS Codes Effective January 1, 2026, CMS. https://www.cms.gov/files/document/annual-update-list-cpt-hcpcs-codes-effective-january-1-2026.pdf
13. Highlights of the 2026 Medicare Physician Fee Schedule Final Rule, NASW, 2025. https://www.socialworkers.org/Practice/Tips-and-Tools-for-Social-Workers/Highlights-of-the-2026-Medicare-Physician-Fee-Schedule-Final-Rule
14. Changes to Medicaid, the ACA and other key provisions of the One Big Beautiful Bill Act, AMA, 2025–2026. https://www.ama-assn.org/health-care-advocacy/federal-advocacy/changes-medicaid-aca-and-other-key-provisions-one-big
15. Medicaid: What to Watch in 2026, KFF, January 23, 2026. https://www.kff.org/medicaid/medicaid-what-to-watch-in-2026/
16. 2026 Outlook: The domino effect of Medicaid cuts, Fierce Healthcare, January 5, 2026. https://www.fiercehealthcare.com/payers/2026-outlook-domino-effect-medicaid-cuts-and-hidden-costs-healthcare
17. 2026 Changes to Medicare & Medicaid, Newsweek, December 30, 2025. https://www.newsweek.com/2026-changes-to-medicare-medicaid-11191542
18. HIPAA Security Rule To Strengthen Cybersecurity of ePHI (NPRM), Federal Register, January 6, 2025. https://www.federalregister.gov/documents/2025/01/06/2024-30983/hipaa-security-rule
19. HIPAA Updates and Changes in 2026, The HIPAA Journal, January 16, 2026. https://www.hipaajournal.com/hipaa-updates-hipaa-changes/
20. Major HIPAA Security Rule Changes on the Horizon, Healthcare Law Insights, February 2026. https://www.healthcarelawinsights.com/2026/02/major-hipaa-security-rule-changes-on-the-horizon/
21. 5 HIPAA Security Rule Changes in 2026, CBIZ, March 2026. https://www.cbiz.com/insights/article/5-hipaa-security-rule-changes-in-2026-and-how-to-prepare
22. Medicare telehealth coverage renewed for two years, AMA, February 2026. https://www.ama-assn.org/practice-management/digital-health/medicare-telehealth-coverage-renewed-two-years
23. What changed in Medicare telehealth under the 2026 spending bill, Medical Economics, March 2026. https://www.medicaleconomics.com/view/what-changed-in-medicare-telehealth-under-the-2026-spending-bill
24. Telehealth FAQ Updated 02/26/2026, CMS. https://www.cms.gov/files/document/telehealth-faq-updated-02-26-2026.pdf
25. Telehealth policy updates, Telehealth.HHS.gov, 2026. https://telehealth.hhs.gov/providers/telehealth-policy/telehealth-policy-updates
26. State of Health AI 2026, Bessemer Venture Partners, January 23, 2026. https://www.bvp.com/atlas/state-of-health-ai-2026
27. 2026 healthcare AI trends: Insights from experts, Wolters Kluwer, December 15, 2025. https://www.wolterskluwer.com/en/expert-insights/2026-healthcare-ai-trends-insights-from-experts
28. AI in health care: 26 leaders offer predictions for 2026, Chief Healthcare Executive, January 15, 2026. https://www.chiefhealthcareexecutive.com/view/ai-in-health-care-26-leaders-offer-predictions-for-2026
29. Top healthcare AI trends in 2026, Healthcare Dive, January 14, 2026. https://www.healthcaredive.com/news/top-healthcare-ai-artificial-intelligence-trends-2026/809493/
30. State of AI in Healthcare and Life Sciences: 2026 Trends, NVIDIA, February 2026. https://blogs.nvidia.com/blog/ai-in-healthcare-survey-2026/
31. Healthcare Predictions 2026, Pabau, March 2026. https://pabau.com/guides/healthcare-predictions-for-2026/
32. How can HHS drive clinical AI adoption?, STAT News, March 2, 2026. https://www.statnews.com/2026/03/02/hhs-clinical-ai-proposal-health-tech-wish-list/
33. Where medical groups are putting new dollars in 2026 budgets, MGMA, 2026. https://www.mgma.com/mgma-stat/where-medical-groups-are-putting-new-dollars-in-2026
34. 2026 Healthcare Revenue Cycle Management Trends, Auxis, 2026. https://www.auxis.com/2026-healthcare-revenue-cycle-management-trends/
35. Revenue Cycle Management Trends Shaping Healthcare in 2026, DrCatalyst. https://www.drcatalyst.com/blog/revenue-cycle-management-trends
36. 6 Healthcare Revenue Cycle Management Trends for 2026, Med USA. https://medusarcm.com/blog/top-revenue-cycle-management-trends-behavioral-health-practices-should-watch-in-2025/
37. Burnout and AI are redefining healthcare work in 2026, Stacker/Indeed, December 9, 2025. https://stacker.com/stories/careers/burnout-and-ai-are-redefining-healthcare-work-2026
38. Practice leaders struggle to unplug heading into 2026, Physicians Practice, December 14, 2025. https://www.physicianspractice.com/view/practice-leaders-struggle-to-unplug-as-stress-levels-surge-heading-into-2026
39. 10 healthcare workforce challenges defining 2026, Becker’s Hospital Review, February 2026. https://www.beckershospitalreview.com/hospital-management-administration/10-healthcare-workforce-challenges-defining-2026/
40. Can staff turnover continue to be tamed in medical practices into 2026?, MGMA, 2026. https://www.mgma.com/mgma-stat/can-staff-turnover-continue-to-be-tamed-in-medical-practices-into-2026
41. Administrative workforce stability: the new clinical metric for 2026, KevinMD, March 2026. https://kevinmd.com/2026/03/administrative-workforce-stability-the-new-clinical-metric-for-2026.html
42. Health Care Workforce: A System Under Pressure, AHA, December 2025. https://www.aha.org/aha-center-health-innovation-market-scan/2025-12-09-health-care-workforce-system-under-pressure-poised-reinvention
43. When health care teams run short, physician burnout rises, AMA, November 2025. https://www.ama-assn.org/practice-management/physician-health/when-health-care-teams-run-short-physician-burnout-rises
44. LEAD (Long-term Enhanced ACO Design) Model, CMS Innovation Center. https://www.cms.gov/priorities/innovation/innovation-models/lead
45. ACO REACH Model Performance Year 2026 Update, CMS. https://www.cms.gov/priorities/innovation/aco-reach-model-performance-year-2026-model-update-quick-reference
46. 2026 CMS Innovation Center Outlook, ATI Advisory. https://atiadvisory.com/resources/2026-cms-innovation-center-outlook/
47. ASM (Ambulatory Specialty Model), CMS Innovation Center. https://www.cms.gov/priorities/innovation/innovation-models/asm
48. ASM Frequently Asked Questions, CMS. https://www.cms.gov/priorities/innovation/asm-ambulatory-specialty-model-frequently-asked-questions
49. The continued evolution of CMS’s mandatory models: The Ambulatory Specialty Model, Milliman. https://www.milliman.com/en/insight/evolution-cms-mandatory-models-ambulatory-specialty-asm
50. Model Overview Factsheet: Ambulatory Specialty Model, CMS. https://www.cms.gov/files/document/asm-model-fact-sheet.pdf
51. New Ambulatory Specialty Model Takes Effect in 2027, ACS/FACS, January 2026. https://www.facs.org/for-medical-professionals/news-publications/news-and-articles/bulletin/2026/january-2026-volume-111-issue-1/new-ambulatory-specialty-model-takes-effect-in-2027/
52. Medical Practice Industry Information You Should Know (Fall 2025), Revele, May 2, 2025. https://www.revelemd.com/blog/medical-industry-news-you-should-know-may-25