We will continue to monitor updates and provide information regarding medical coding and billing for COVID-19. Here we cover CPT coding, diagnosis codes, lab codes, reimbursement rates, and restrictions and requirements tied to telehealth and coronavirus testing.
Quick Links
Use the links below to navigate to sections of this article.
- Summary of Medicare Telemedicine Services
- Virtual Check-In
- E-Visits and Telehealth
- Can All Providers Perform Telehealth Services or Just Physicians?
- CPT Coding
- FQHC/RHC Guidance
- Coronavirus Testing
- Televisit Documentation Requirements
- Diagnosis Codes
- Lab Codes
- Reimbursement Rates
- Catastrophic Plans
- Reimbursement Details and Claim Requirements
Information in this article is subject to change. We will continue to update this article as additional information becomes available. This article was last revised Thursday, August 6, 2020 at 12:40 pm Central.
Summary of Medicare Telemedicine Services
Click here for a complete list of HCPC/CPT codes for Medicare Telehealth Visits.
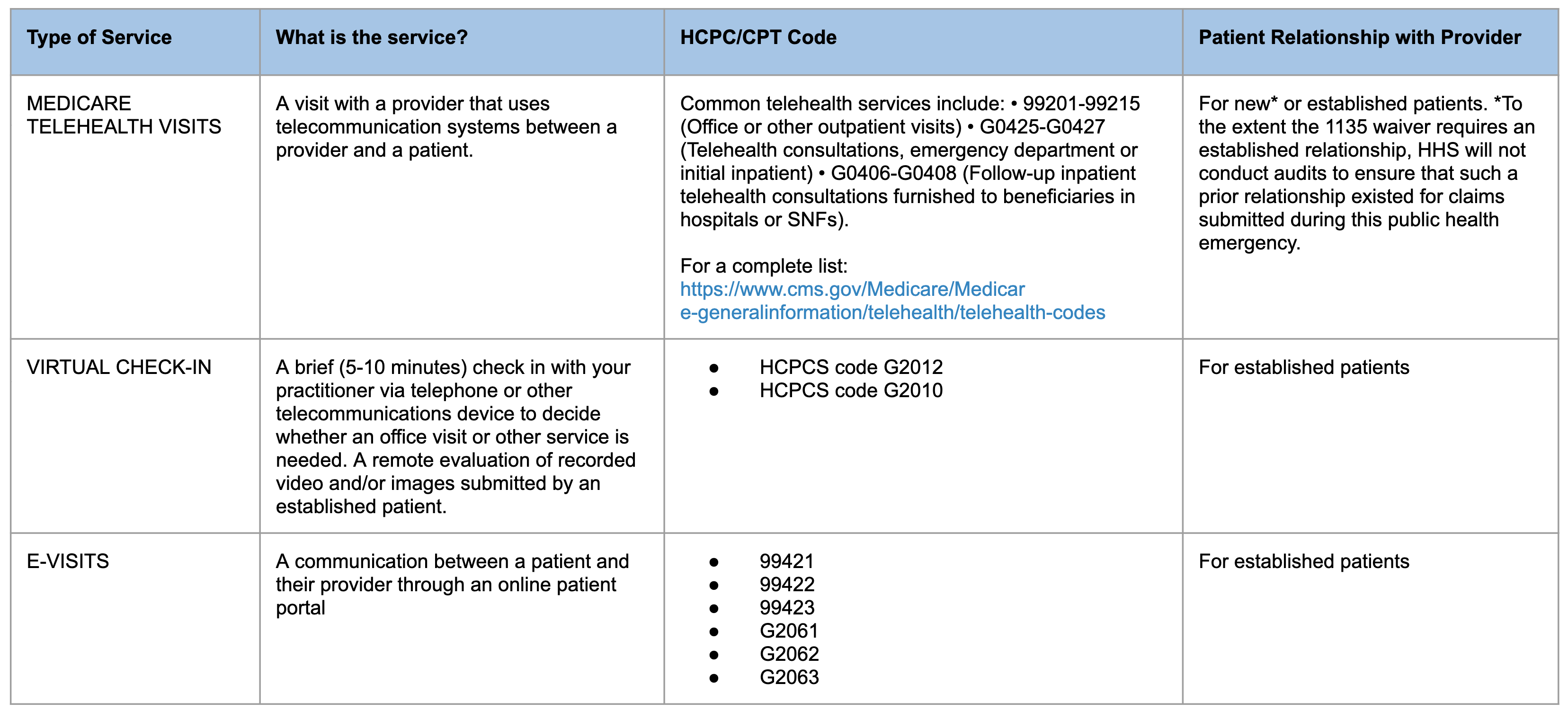
Medicare Telehealth Visit
A medicare telehealth visit is a visit with a provider that uses telecommunication systems between a provider and a patient. Common telehealth service HCPC/CPT Codes include:
- 99201-99215: Office or other outpatient visits
- G0425-G0427: Telehealth consultations, emergency department, or initial inpatient
- G0406-G0408: Follow-up inpatient telehealth consultations furnished to beneficiaries in hospitals or SNFs.
Medicare telehealth visits can be used for established or new — patients to the extent the 1135 waiver requires an established relationship, HHS will not conduct audits to ensure such a prior relationship existed for claims submitted during this public health emergency.
Virtual Check-in
Virtual check-ins are brief (5-10 minutes) check-in with a practitioner via telephone or other telecommunications devices to divide whether an office visit or other service is needed. A remote evaluation of recorded video and/or images submitted by an established patient. Common virtual check-in HCPC/CPT Codes include:
- HCPCS code G2012
- HCPCS code G2010
Virtual check-ins are for established patient relationships.
E-Visits
E-visits is a communication between a patient and their provider through an online patient portal. E-visit HCPC/CPT Codes include:
- 99421
- 99422
- 99423
- G2061
- G2062
- G2063
E-visits are for established patient relationships.
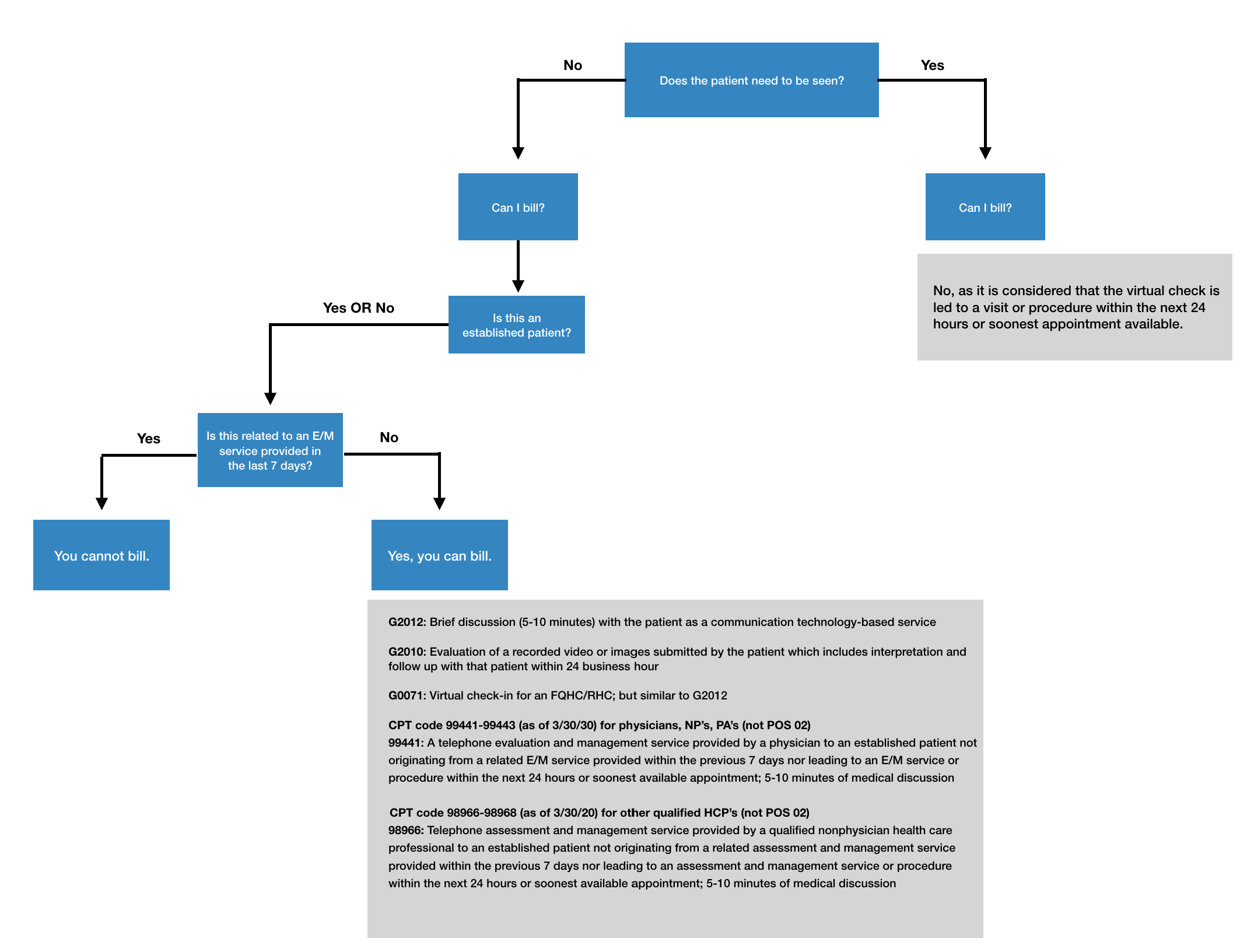
Virtual Check-In Billing Flowchart
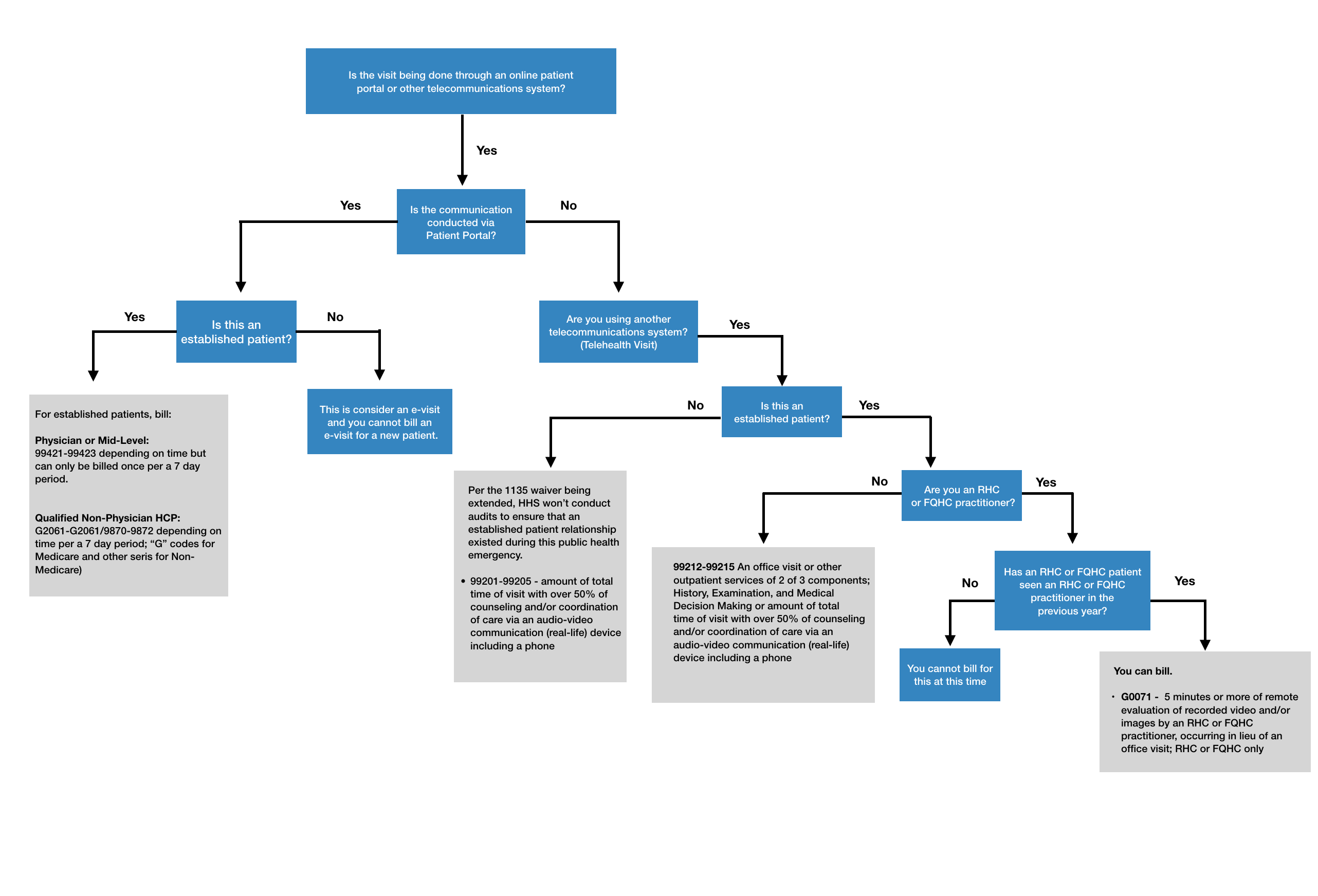
E-Visits and Telehealth Billing Flowchart
Can All Providers Perform Telehealth Services or Just Physicians?
Telehealth eligible providers' specialties include:
|
|
It’s standard for telehealth that providers must be licensed in the state in which he/she is rendering services. But on 3/18/20, Vice President Mike Pence announced that the Department of Health and Human Services will issue a regulation that allows medical professionals to practice in states where they are not licensed.
What is an Originating Site?
An originating site authorized by law includes:
|
|
Though Telehealth visits typically include an originating site, CMS is waiving the requirement therefore patients can receive telehealth services in their home. In addition, Telehealth visits are usually limited to patients in rural areas but CMS has waived this requirement.
What is a Distant Site?
Though subject to state law, distant sites include:
|
|
A medical professional is not required to present the beneficiary to the physician or practitioner unless it is medically necessary. The decision of medical necessity is made by the physician or practitioner at the distant site.
CPT Coding
Do I Use Different E&M Codes for Telehealth/Virtual-based Visits?
The codes that will be billed for what Medicare actually defines as Medicare “telehealth services” will typically be standard E&M office visit codes (such as 99213, 99214) along with a telehealth place of service, and potentially a modifier (if required by commercial payers).
Please use this link for telehealth service CPT/HCPCS codes.
The Medicare “communications-based technology” codes are split into two different service types known as Virtual Check-In or E-Visits. Neither of these visits are deemed by CMS to be Medicare “telehealth services” which means they are not subject to the typical statutory restrictions regarding the originating site or rural geography, though CMS has lifted these during this public emergency situation. These services can be furnished in the patient's home, regardless of a national emergency declaration.
A virtual check-in is a brief (5-10 minutes) communication initiated by the patient with a practitioner via telephone or other telecommunications device to determine if an office visit is needed. Virtual check-in’s do require an established patient relationship (seen by the provider within the last three years) which hasn’t been waived by CMS due to this public health emergency. A virtual check-in cannot be related to a medical visit within the previous seven days and does not lead to a medical visit within the next 24 hours (or the soonest appointment available). The virtual check-in codes are:
- G2012: Brief communication technology-based service by a physician or other qualified health professional who can report evaluation and management services, provided to an established patient, not originating from a related E/M service provided within the previous seven days nor leading to an E/M service or procedure within the next 24 hours or soonest appointment available; 5-10 minutes or medical discussion
- G2010: Remote evaluation of a recorded video and/or images submitted by an established patient, including interpretation and follow-up with the patient within 24 business hours, not originating from a relation E/M service provided within the previous seven days nor leading to an E/M service within the next 24 hours or soonest available appointment.
- 99441: Telephone evaluation and management service by a physician or other qualified health care professional who may report evaluation and management services provided to an established patient, parent, or guardian not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment; 5-10 minutes of medical discussion
- 98966: Telephone assessment and management service provided by a qualified non-physician health care professional to an established patient, parent, or guardian not originating from a related assessment and management service provided within the previous 7 days nor leading to an assessment and management service or procedure within the next 24 hours or soonest available appointment; 5-10 minutes of medical discussion
- G0071: Payment for communication technology-based services for 5 minutes or more of a virtual (non-face-to-face) communication between a Rural Health Clinic (RHC) or Federally Qualified Health Center (FQHC) practitioner and RHC or FQHC patient, or 5 minutes or more of remote evaluation of recorded video and/or images by an RHC or FQHC practitioner, occurring in lieu of an office visit; RHC or FQHC only
E-visits are different from telehealth visits because they must occur through an online patient portal. This service is non-face-to-face; both MDs and mid-levels are eligible to bill for this service. This code series is also time-based and specific documentation requirements must be met.
99421 |
Online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 5-10 minutes. |
99422 |
Online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 11-20 minutes. |
99423 |
Online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 21 or more minutes. |
99421, 99422, and 99243 can only be billed once per 7 days. You will see in the code description that states the time is cumulative - your provider can sum up the time spent with the patient and bill accordingly. Note, that the provider can not include time spent with other services with these codes. Services can not be billed on the same day as an office visit or consult. This service is not billable if the patient was treated within 7 days of the E/M for the same symptom.
E-Visits by a Qualified Non-Physician Health Care Professional
|
Medicare |
Non-Medicare |
Description |
|
G2061 |
98970 |
Qualified non-physician health care professional online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 5-10 minutes |
|
G2062 |
98971 |
Qualified non-physician health care professional online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 11-20 minutes |
|
G2063 |
98972 |
Qualified non-physician health care professional online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 21 or more minutes |
Are Wellness Visits Eligible to Be Done and Reimbursed Through Telehealth/Virtual-Based Services?
Since preventive visit codes such as 99391 - 99397 aren’t reimbursed by CMS, they haven’t addressed these types of visits. However, we are finding certain carriers are stating that they will cover well visits to be completed and billed through telehealth. An example is CareFirst BCBS. Please see below:
https://individual.carefirst.com/carefirst-resources/pdf/carefirst-telemedicine-code-modifier.pdf
Are you an FQHC or RHC?
Specific to Telehealth or e-Visits
Effective April 17, 2020 RHCs and FQHCs can perform and bill telehealth services and e-Visits as a distant site. The reimbursement will be at the all-inclusive rate (AIR) for RHCs and FQHCs will be paid at their prospective payment system rate (PPS). Modifiers 95 and CS will be valid. For correct CPT coding, please see: https://www.cms.gov/files/document/se20016.pdf
Specific to Virtual Check-ins
Effective January 1, 2019, FQHCs & RHCs can receive payment for virtual check-in services when:
- At least 5 minutes of communication technology-based or remote evaluation services are furnished
- An FQHC/RHC practitioner provides virtual communication service to a patient who has had an FQHC/RHC billable visit within the previous year
- The medical discussion or remote evaluation is for a condition not related to an FQHC/RHC service provided within the previous 7 days, and does not lead to an FQHC/RHC visit within the next 24 hours or at the soonest available appointment.
- Use HCPCS code G0071 (Virtual Communication Services) either alone or with other payable services.
- See Virtual Communication Services Frequently Asked Questions (PDF)
See Telehealth Coverage Policies in the time of COVID-19 to Date: Center for Connected Health Policy
What CPT/HCPCS Codes Do I Use for Coronavirus Testing? Are These Codes Accepted by All Payers?
Laboratory Codes
- U0001: 2019 Novel Coronavirus Real Time RT-PCR Diagnostic Panel: To be used when the specimen is sent to the CDC or a CDC-approved local/state health department laboratory (effective 4/1/20)
- U0002: 2019-nCoV Coronavirus, SARS-CoV-2/2019-nCoV (COVID-19), any technique, multiple types or subtypes (includes all targets), non-CDC: To be used when specimens are sent to commercial laboratories e.g. Quest or LabCorp, and not to the CDC or CDC-approved local/state health department laboratories (effective 4/1/20)
- 87635: SARS-COV-2 COVID-19 AMP/PRB (effective 3/13/20)
- G2023: Independent labs report this code when a trained laboratory technician collects a nasopharyngeal, oropharyngeal, sputum, or another type of specimen for the purpose of performing a laboratory test for the SARS–CoV–2 virus.
- G2024: Specimen collection for severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) (coronavirus disease [COVID-19]) from an individual in an SNF or by a laboratory on behalf of a Home Health Agency, any specimen source.
Specimen Transfer
If you are collecting the specimen and sending it to a lab for processing, please use code:
- 99000: Handling and/or conveyance of specimens for transfer from the physician’s office to an outside laboratory.
- 99001: Handling and/or conveyance of specimens for transfer from collection outside of the office to the laboratory.
- 99211: for swabs collected in office or group practice’s testing site. Append modifier 25 if same day as assessment.
Would I Use a Modifier?
A new modifier has been, CS, which is to be added to Medicare claims for COVID-19-related diagnosis and testing.
Are These Codes (Telehealth, Virtual-based Visits, and Coronavirus Testing) in my eClinicalWorks System with Billed Fees Attached?
If these codes are not present in your system or do not have fees attached, and you are a Revele client, please contact your Client Success Team and we will assist with getting this information added.
Televisit Documentation Requirements
Documentation Requirements: The televisits (Telehealth, Virtual Check-ins, and e-Visits) should be documented in the medical record.
Minimum required documentation elements include:
- Notation of the patient’s initiation and verbal or written consent to the televisit
- Providers may contact patients to inform of the new televisits’ rules, upon the patient’s consent, the provider can provide health care during the same call.
- Names of all people present during a televisit and their role
- Chief complaint or reason for the televisit
- Relevant history, background, and/or results
- Assessment
- Plan of care or next steps
- Total time spent of the televisit service
Diagnosis Codes
Are Any Diagnosis Codes Excluded From Coverage for Telehealth/Virtual-based Visits?
Not all conditions, injuries, and illnesses can be treated or addressed in a telehealth/virtual-based encounter due to limited visualization. It is the provider’s responsibility to determine if a telehealth/virtual-based service is acceptable health care per the patient’s complaint.
What Diagnosis Codes Do I Use for Coronavirus Testing?
Exposure
- Z03.818: Encounter for observation for suspected exposure to other biological agents ruled out. To be used where there’s a concern about a possible exposure to COVID-19 but this is ruled out after evaluation
- Z20.828: Contact with and suspected exposure to other viral communicable diseases. To be used when there is an actual exposure to someone who is confirmed to have COVID-19
Signs and Symptoms
For patients presenting with any signs/symptoms and a definitive diagnosis hasn’t been established, assign the appropriate code(s) for each of the presenting signs and symptoms:
- Cough: R05
- Fatigue: R53.83
- Fever: R50.9
- Sore throat: J02.9
Concern Cases
Z71.84:
- Encounter for health counseling related to travel
- Encounter for health risk and safety counseling for (international) travel
Z71.1:
- Person with feared health complaint in whom no diagnosis is made
- Person encountering health services with feared condition which was not demonstrated
- Person encountering health services in which problem was normal state
Worried well Excludes1: medical observation for suspected diseases and conditions proven not to exist (Z03.-)
Screening Cases
- Z11.59: Encounter for screening for other viral diseases
Confirmed cases
- Prior to 4/1/2020, report the code for the patient’s condition that is related to the COVID-10 (example J12.890-other viral pneumonia) and B97.29-Other coronavirus as the cause of diseases classified elsewhere
- U07.1: 2019-nCoV acute respiratory disease (effective 4/1/2020)
Are These Codes (Telehealth and Coronavirus Testing) in my eClinicalWorks System with Billed Fees Attached?
The diagnosis codes should be present in your system unless the code has just been released. If you are unable to find them, please contact your Client Success Team for assistance.
If you utilize Intelligent Medical Objects (IMO) a.k.a. SmartSearch within your system to help you select the most appropriate diagnosis codes, please view this link regarding updated descriptions for 2019 n-CoV.
Lab Codes
Is There a Coronavirus Lab Test Built in my eClinicalWorks system? Is the Test Linked to the Right CPT/HCPCS Codes?
If you have never performed testing for the coronavirus the test may not be built in your system. This test will need to be added with the appropriate CPT code attached as well as the applicable lab codes. If you are a Revele client and need assistance getting this test added, please reach out to your Client Success Team for assistance.
Reimbursement Rates
What are the Average Reimbursement Rates for Telehealth/Virtual-based Visits From Major Carriers Such as Medicare, BCBS, Cigna, Humana, etc.?
The rates vary based on payer, specifically with commercial carriers as they are based on your contract negotiated rate.
Medicare: The payment is 80 percent of the Medicare PFS facility amount for the distant site service.
Patients pay 20% of the Medicare-approved amount for your doctor or other health care provider’s services, and the Part B deductible applies. For most telehealth services, patients will pay the same amount that they would if they received the services in person.
On April 30, 2020, CMS announced that telephone E/M services (99441 - 99443) will approach nearly a 200% reimbursement increase during the COVID-19 public health emergency. The reimbursement rate range for this code set used to be $14 - $41 but the reported increase will create a range of $46 - $110.
Blue Cross Blue Shield Association: Recently announced that its network of 36 independent and locally operated Blue Cross and Blue Shield companies will expand access to telehealth and nurse/provider hotlines. This applies to fully insured, individual, and Medicare Advantage plan members and plans are working with state Medicaid and CHIP agencies to ensure people have access to necessary testing and other services.
Cigna: Cigna customers, pertaining to the coronavirus (COVID-19), will waive all co-pays or cost-shares to help fight the rapid spread of the virus in the U.S. and for its globally mobile customers.
Highmark: Claims for virtual PCP visits are submitted based on how you are contracted with Highmark. Reimbursement will be based on the current plan allowance in place at the time services were rendered. Member cost-sharing (copay, deductible, and/or coinsurance) and visit limits apply if applicable. For more information on billing and reimbursement, please see Highmark Reimbursement.
Blue Shield California: For information regarding Blue Shield California, please visit the Blue Shield CA coronavirus page: https://news.blueshieldca.com/2020/03/06/update-members-coronavirus
Humana: For information regarding Humana, please visit the Humana coronavirus page: https://www.humana.com/provider/coronavirus
UHC (Commercial, Medicare Advantage, Medicaid-based products): Effective 3/17/20 through 4/30/20 (though subject to be extended), UHC will reimburse for telehealth and virtual-based visits for patients whose benefit plans cover these services. The update is that they are following CMS’s policy during this timeframe to lift the originating site restriction.
Magellan Behavioral Health: During this crisis, Magellan is waiving their normal protocols to allow providers to provide and bill sessions by telephone. Though authorization requirements are still in place at this time.
Medicaid: We are commonly being asked for state Medicaid guidelines. The best resource to use to identify if your state has additional exceptions for accepting the blanket waiver can be found at medicaid.gov here.
What are the Average Reimbursement Rates for Coronavirus Testing From Major Carriers Such as BCBS, UHC, Cigna, Aetna, etc.?
These rates are to be determined from commercial payers.
Medicare:
- Medicare covers the lab tests for COVID-19. The patient pays no out-of-pocket costs. As of 3/19/20 CMS announced that the test through the CDC will be reimbursed at $36 with tests from other entities being reimbursed at $51. However, prices may slightly vary depending on the provider's local Medicare Administrative Contractor (MAC)
- At this time, there's no vaccine for COVID-19. However, if one becomes available, it will be covered by all Medicare Prescription Drug Plans (Part D).
- If you have a Medicare Advantage Plan, you have access to these same benefits. Medicare allows these plans to waive cost-sharing for COVID-19 lab tests. Many plans offer additional telehealth/virtual-based benefits beyond the ones described.
Blue Cross Blue Shield: Recently announced that their network of 36 independent and locally operated Blue Cross and Blue Shield companies will waive prior authorizations for diagnostic tests and covered services for COVID-19 and cover those tests at no cost share to members. This applies to fully insured, individual, and Medicare Advantage plan members and plans are working with state Medicaid and CHIP agencies to ensure people have access to needed testing and services.
UHC: UnitedHealthcare will cover testing for Coronavirus (COVID-19) at approved locations for insured, Medicaid, and Medicare members.
Cigna: Cigna customers will have access to coronavirus (COVID-19) testing, as prescribed by health practitioners, and the company will waive all co-pays or cost-shares to help fight the rapid spread of the virus in the U.S. and for its globally mobile customers. At this time, Cigna is stating this will apply through May 31, 2020.
Aetna: Aetna will cover the cost of physician-ordered testing for patients who meet CDC guidelines, which can be done in any approved laboratory location. Aetna will waive the member costs associated with diagnostic testing at any authorized location for all commercial, Medicare and Medicaid lines of business. For more information, visit Aetna's coronavirus resources.
Catastrophic Plans
What is a Catastrophic Plan?
Designed to have low premiums but still protect its enrollees from substantial medical debt if they suffer a catastrophic illness.
Do Catastrophic Plans Cover the Diagnosis and Treatment of COVID-19?
Yes, they must cover essential health benefits (EHB) as required by the Patient Protection and Affordable Care Act (PPACA) but are typically subject to limitations. The specific coverage details and enrollee cost-sharing varies by plan with some requiring prior authorizations to be obtained before services are eligible for coverage.
Will the Department of Health and Human Services Allow Issuers of Catastrophic Plans to Provide Coverage Even if an Enrollee’s Deductible Hasn’t Been Met?
Yes, the Department of Health and Human Services won’t be taking action against any health issuer that amends their catastrophic plans to provide pre-deductible coverage for services related to the diagnosis and treatment of COVID-19.
Will There Be Funding to Cover Uninsured Patients for COVID-19 Diagnosis/Treatment-related Costs?
Yes, uninsured patients will be covered for COVID-19 diagnosis and treatment related costs through funding from the Family First Coronavirus Response Act. Learn more about the HRSA COVID-19 Uninsured Program.
Reimbursement Details and Claim Requirements
Will Patients Owe a Copay for Telehealth/Virtual-based Services?
Many plans are saying they are waiving copays until further notice.
- Medicare: Per CMS, the anti-kickback rule for any services paid by Medicare, Medicaid, or CHIP will not be enforced in regards to telehealth visits. This means that providers can reduce or waive cost-sharing for telehealth visits without penalty but they aren’t required to waive the fees.
- Aetna: For the next 90 days, Aetna will offer zero co-pay telemedicine visits – for any reason
- Humana: Currently waiving member cost share for urgent care telehealth visits over the next 90 days. Because of this, you shouldn’t collect payment from Humana Medicare Advantage, Medicaid, and Commercial HSA patients for these services. Humana will issue further information on how to determine if other ASO group-sponsored plans have opted out of cost-share waivers. In the meantime, please use your best judgment.
Can I Provide Telehealth/Virtual-based Services to All Patients and Be Reimbursed or Do They Have to Be Experiencing Symptoms of the Coronavirus/High-risk Patients?
Per CMS, during this Public Health Emergency, they will not enforce the prior-relationship requirement for telehealth/virtual-based visits.
With symptoms related to the Coronavirus:
- The patient must verbally consent to using virtual check-ins and the consent must be documented in the medical record prior to the patient using the service.
- The communication between the patient and physician is not related to a medical visit within the previous 7 days and does not lead to a medical visit within the next 24 hours (or soonest appointment available).
Are Telehealth Documentation Requirements the Same as a Face-to-face Encounter?
All that is seen, communicated, discussed, and treated should reflect in the medical record documentation.
What Place of Service Do I bill for Telehealth/Virtual-based Visits?
The correct place of service for telehealth is 02 for visits considered telehealth, otherwise use POS 11 if conducted in an office setting (or other POS based on setting). Essentially, if the services would have been provided in person had this emergency not been going on, you will bill the place of service based on where it would have occurred, example: POS 11. But, if it’s a true telehealth service, bill POS 02.
What Modifiers Do I Use?
- Modifier 95 - Synchronous Telemedicine Service Rendered Via a Real-Time Interactive Audio and Video Telecommunications System. Append modifier 95 with E/M codes 99201-99215.
- Modifier GQ - Services provided via asynchronous telecommunications system
- Modifier GT - Services provided via interactive audio and video telecommunications systems
- Modifier G0 (G–zero) denotes that a provider diagnosed, evaluated, or treated a patient for an acute stroke remotely using an audio and/or video telecommunication system.
Can Claims Be Submitted Now for Coronavirus Testing or Do They Need to Be Held?
CMS was ready to accept claims as of 4/1/2020 for dates of service effective 2/4/20 and forward (until further notice).
Information in this article is subject to change. We will continue to update this article as additional information becomes available.
A/R OPTIMIZATION SERVICE
Speed-up payments with A/R Fuel
Quickly convert aged A/R into cash flow.